
Severe MAS & APHN: The Advanced Management Protocol
Severe MAS & APHN:
The Advanced Management Protocol
Evidence-based pathways for Meconium Aspiration Syndrome and Acute Pulmonary Hypertension of the Newborn.
The Pathophysiological Cascade
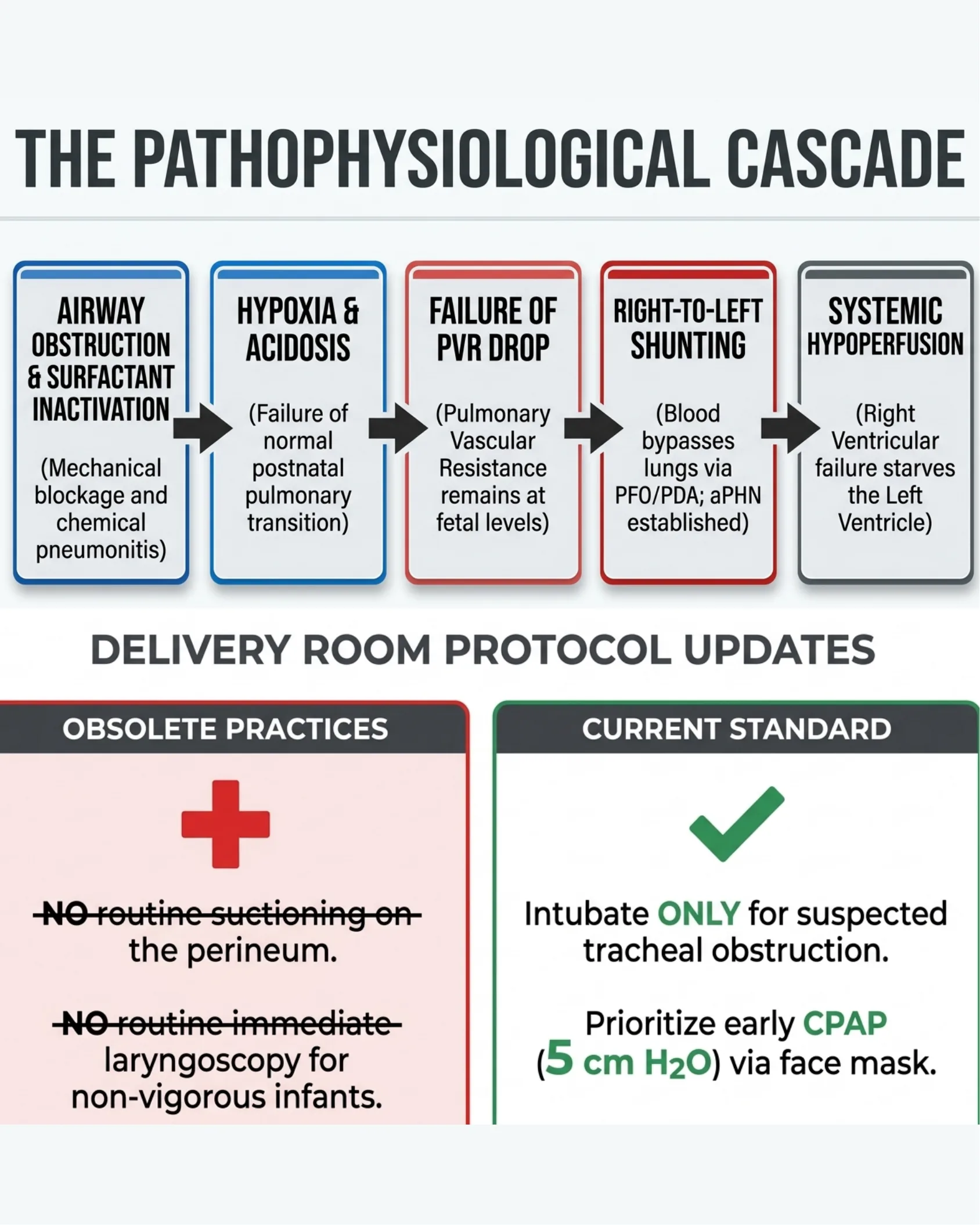
The Pathophysiological Cascade
- Airway Obstruction & Surfactant Inactivation — (Mechanical blockage and chemical pneumonitis)
- Hypoxia & Acidosis — (Failure of normal postnatal pulmonary transition)
- Failure of PVR Drop — (Pulmonary Vascular Resistance remains at fetal levels)
- Right-to-Left Shunting — (Blood bypasses lungs via PFO/PDA; aPHN established)
- Systemic Hypoperfusion — (Right Ventricular failure starves the Left Ventricle)
Delivery Room Protocol Updates
| Obsolete Practices | Current Standard |
|---|---|
| Intubate ONLY for suspected tracheal obstruction. | |
| Prioritize early CPAP (5 cm H2O) via face mask. |
The Diagnostic Anchors for aPHN
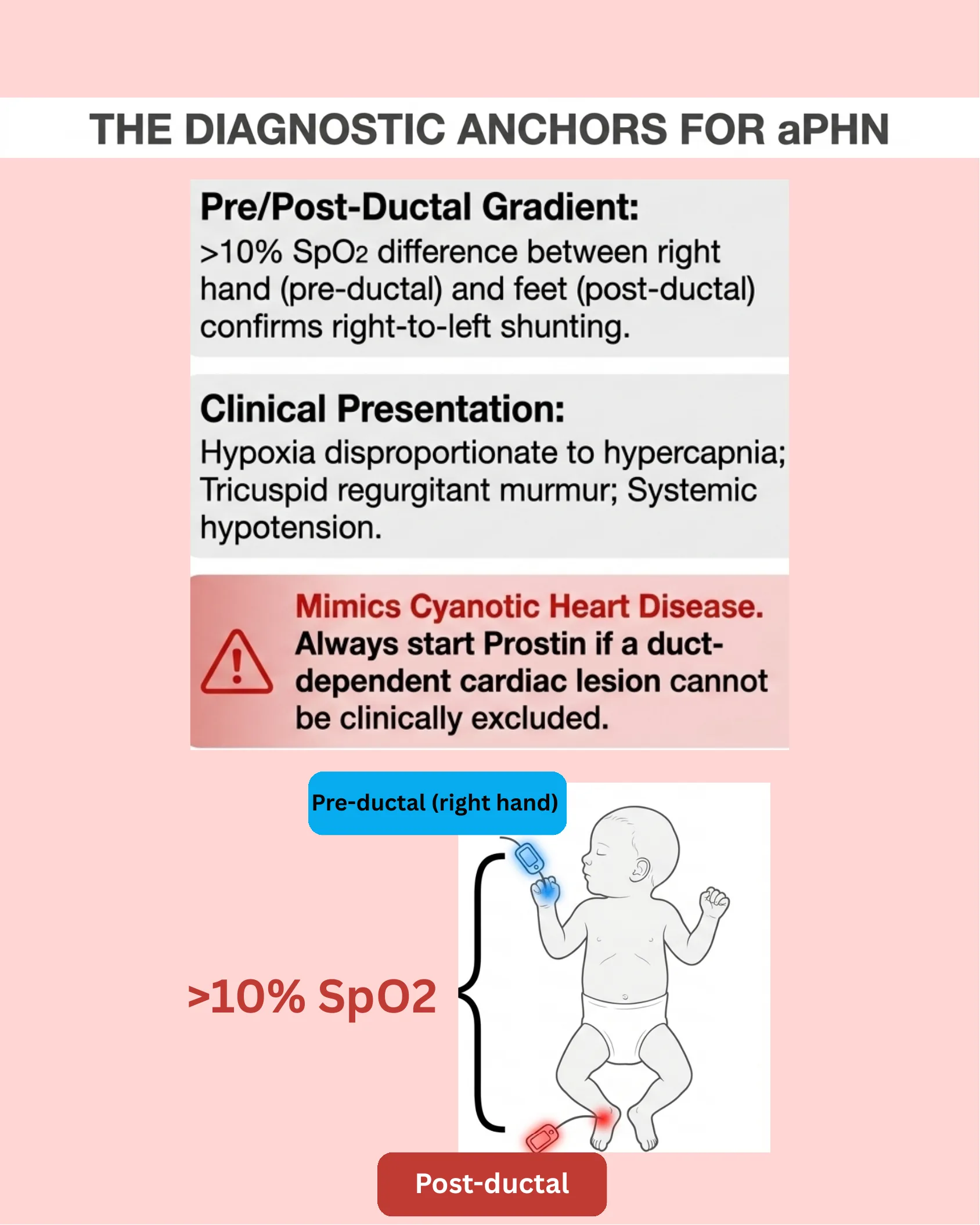
The Diagnostic Anchors for aPHN
Pre/Post-Ductal Gradient: >10% SpO2 difference between right hand (pre-ductal) and feet (post-ductal) confirms right-to-left shunting.
Clinical Presentation: Hypoxia disproportionate to hypercapnia; Tricuspid regurgitant murmur; Systemic hypotension.
Mimics Cyanotic Heart Disease. Always start Prostin if a duct-dependent cardiac lesion cannot be clinically excluded.
- Pre-ductal (right hand)
- >10% SpO2 difference
- Post-ductal
The Critical Role of TnECHO
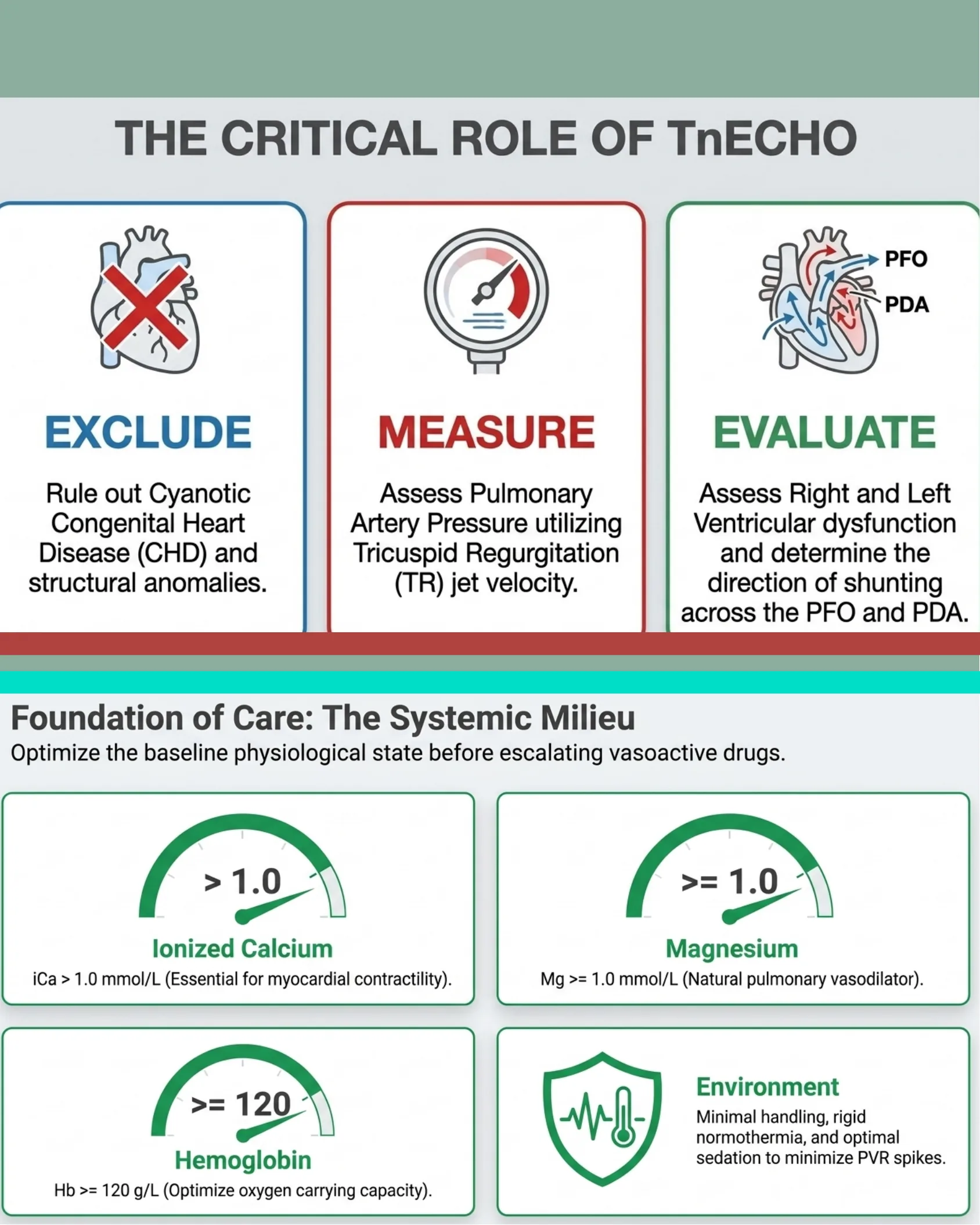
The Critical Role of TnECHO
- Exclude — Rule out Cyanotic Congenital Heart Disease (CHD) and structural anomalies.
- Measure — Assess Pulmonary Artery Pressure utilizing Tricuspid Regurgitation (TR) jet velocity.
- Evaluate — Assess Right and Left Ventricular dysfunction and determine the direction of shunting across the PFO and PDA.
Foundation of Care: The Systemic Milieu
Optimize the baseline physiological state before escalating vasoactive drugs.
- Ionized Calcium: > 1.0 mmol/L (Essential for myocardial contractility).
- Magnesium: >= 1.0 mmol/L (Natural pulmonary vasodilator).
- Hemoglobin: >= 120 g/L (Optimize oxygen carrying capacity).
- Environment: Minimal handling, rigid normothermia, and optimal sedation to minimize PVR spikes.
Respiratory Strategy: Gentle Ventilation
Respiratory Strategy: Gentle Ventilation
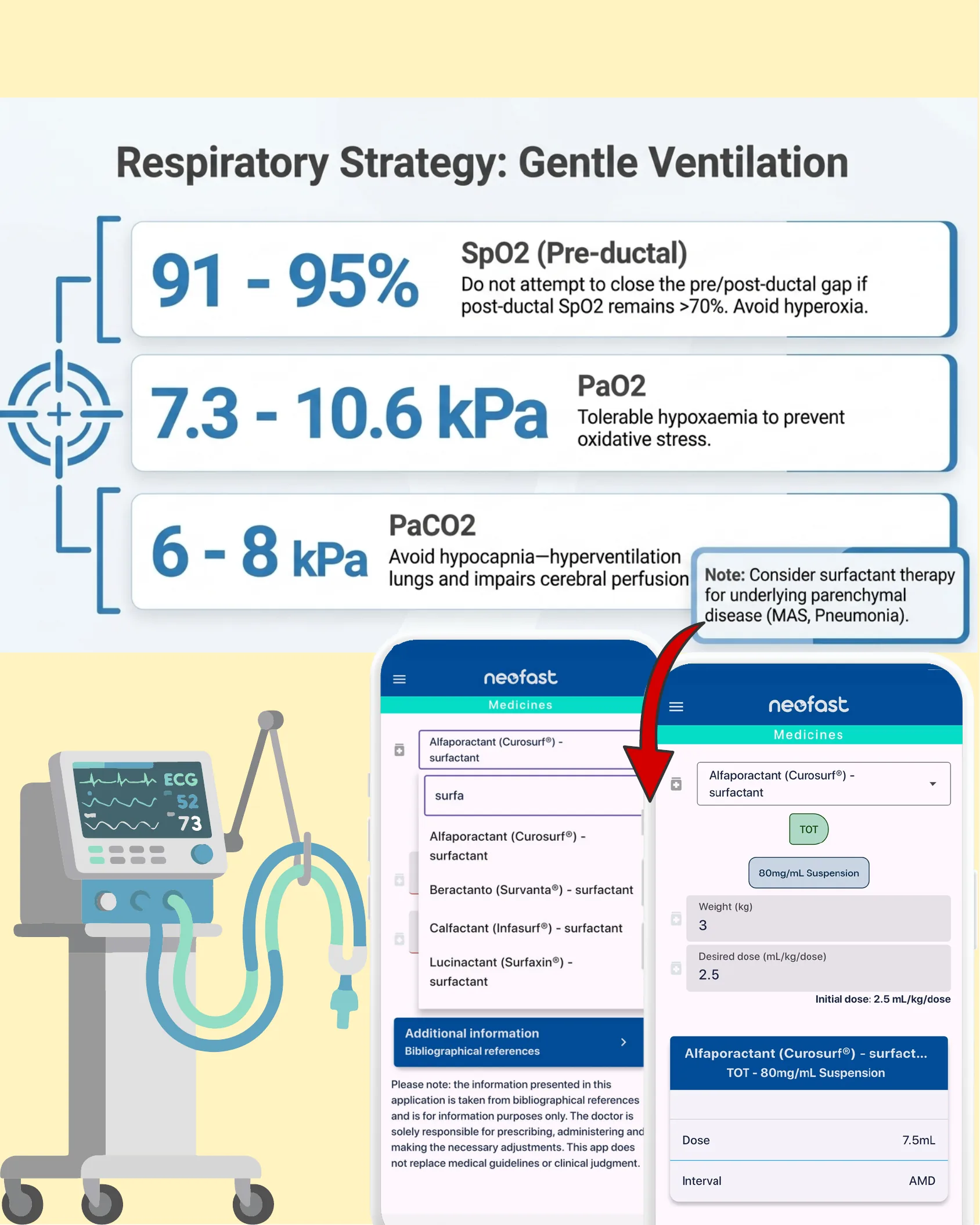
- SpO2 (Pre-ductal): 91–95% — Do not attempt to close the pre/post-ductal gap if post-ductal SpO2 remains >70%. Avoid hyperoxia.
- PaO2: 7.3–10.6 kPa — Tolerable hypoxaemia to prevent oxidative stress.
- PaCO2: 6–8 kPa — Avoid hypocapnia—hyperventilation lungs and impairs cerebral perfusion.
Note: Consider surfactant therapy for underlying parenchymal disease (MAS, Pneumonia).
App screenshot (Neofast Medicines): Alfaporactant (Curosurf®) – surfactant; search field “surfa”; options: Alfaporactant (Curosurf®) – surfactant, Beractanto (Survanta®) – surfactant, Calfactant (Infasurf®) – surfactant, Lucinactant (Surfaxin®) – surfactant.
- Route: TOT
- Formulation: 80mg/mL Suspension
- Weight (kg): 3
- Desired dose (mL/kg/dose): 2.5
- Initial dose: 2.5 mL/kg/dose
- Dose: 7.5mL
- Interval: AMD
Disclaimer: Please note: the information presented in this application is taken from bibliographical references and is for information purposes only. The doctor is solely responsible for prescribing, administering and making the necessary adjustments. This app does not replace medical guidelines or clinical judgment.
Tracking the Oxygenation Index (OI)
Tracking the Oxygenation Index (OI)
Airway/Blue — Vascular/Red spectrum
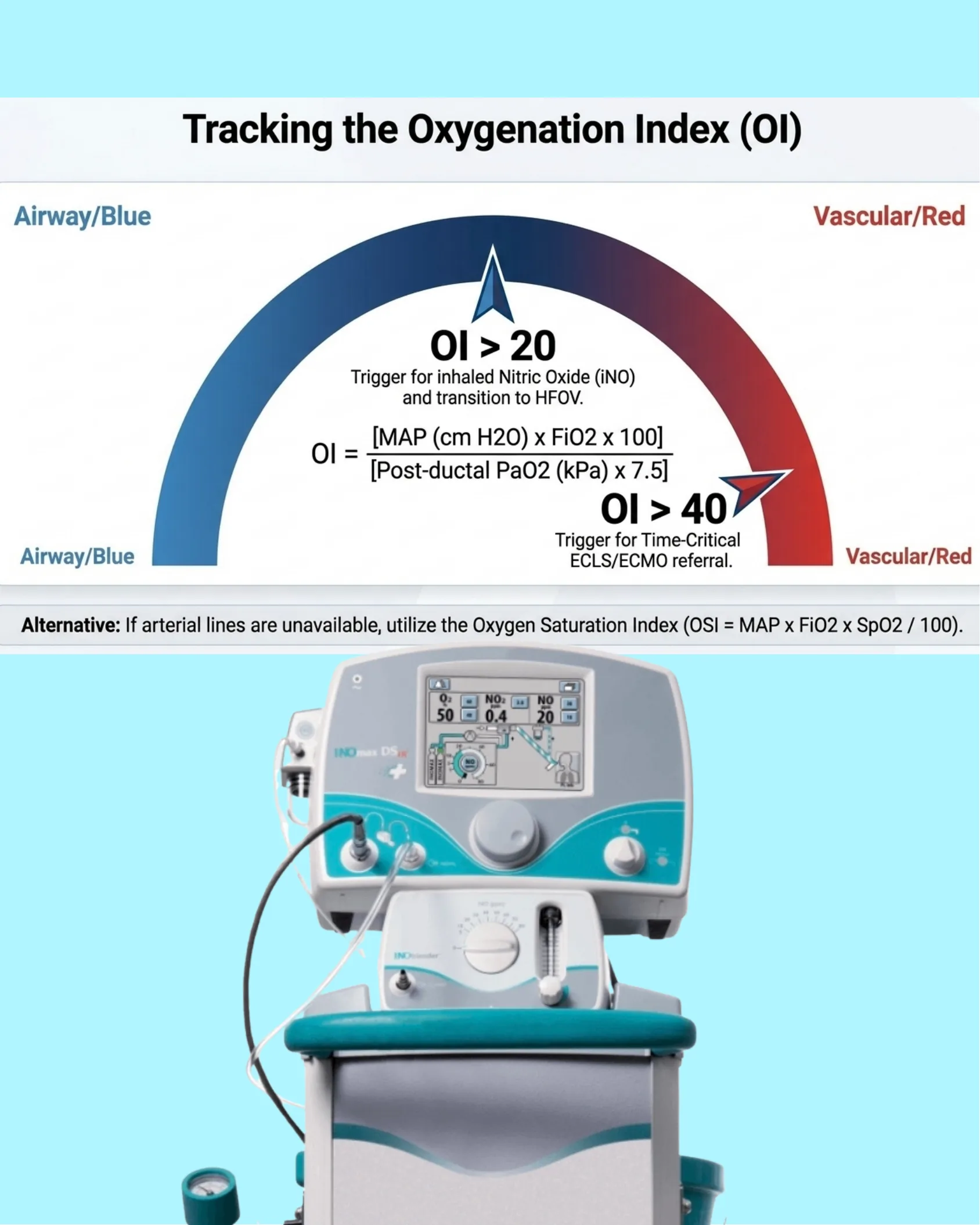
OI Formula: OI = [MAP (cm H2O) x FiO2 x 100] / [Post-ductal PaO2 (kPa) x 7.5]
- OI > 20 — Trigger for inhaled Nitric Oxide (iNO) and transition to HFOV.
- OI > 40 — Trigger for Time-Critical ECLS/ECMO referral.
Alternative: If arterial lines are unavailable, utilize the Oxygen Saturation Index (OSI = MAP x FiO2 x SpO2 / 100).
Device shown: INOmax DSIR nitric oxide delivery system with INOblender, displaying Q2 50, NO2 0.4, NO 20 settings.
Escalation to HFOV
Escalation to HFOV
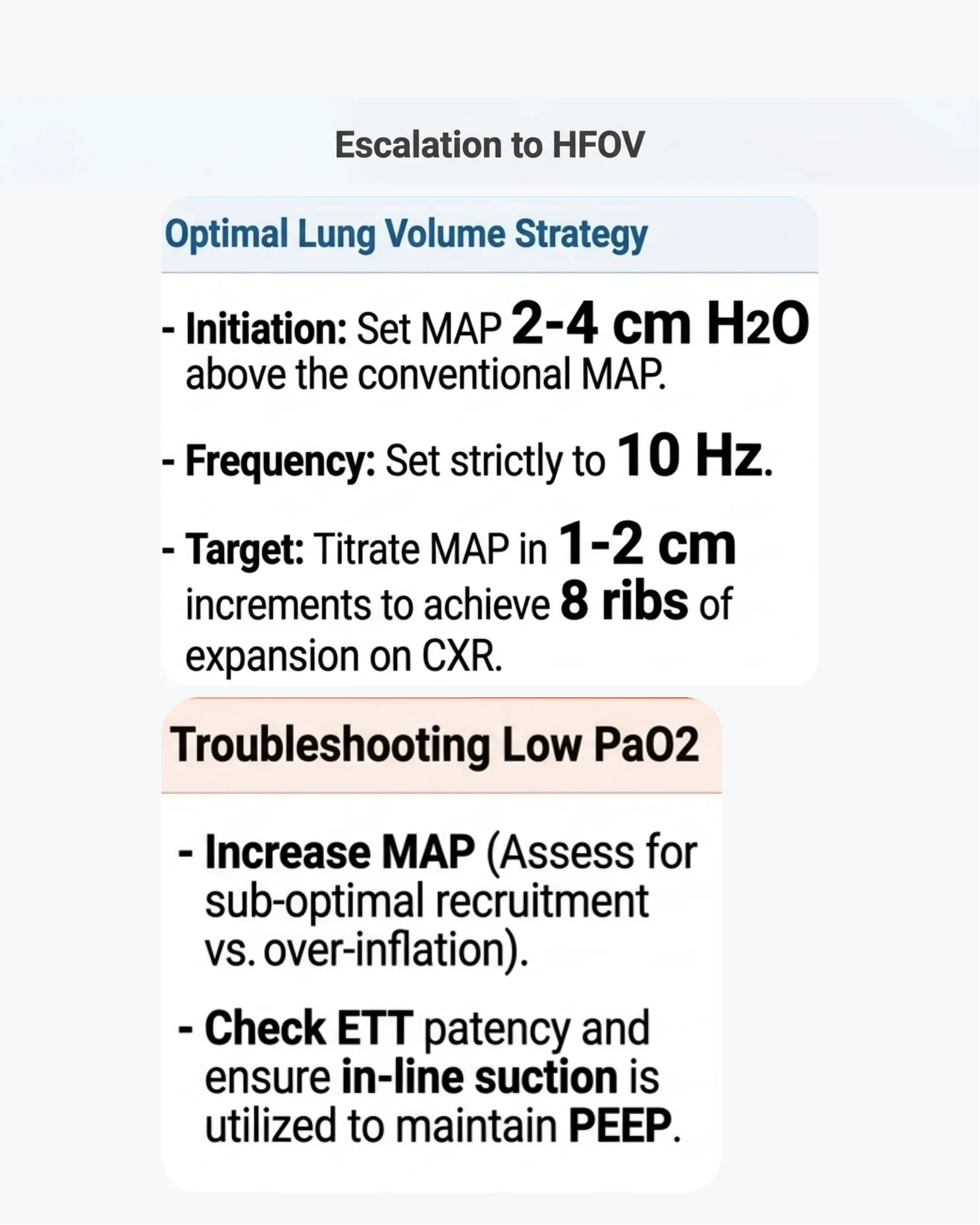
Optimal Lung Volume Strategy
- Initiation: Set MAP 2-4 cm H2O above the conventional MAP.
- Frequency: Set strictly to 10 Hz.
- Target: Titrate MAP in 1-2 cm increments to achieve 8 ribs of expansion on CXR.
Troubleshooting Low PaO2
- Increase MAP (Assess for sub-optimal recruitment vs. over-inflation).
- Check ETT patency and ensure in-line suction is utilized to maintain PEEP.
Targeted Pulmonary Vasodilation: iNO Protocol
Targeted Pulmonary Vasodilation: iNO Protocol
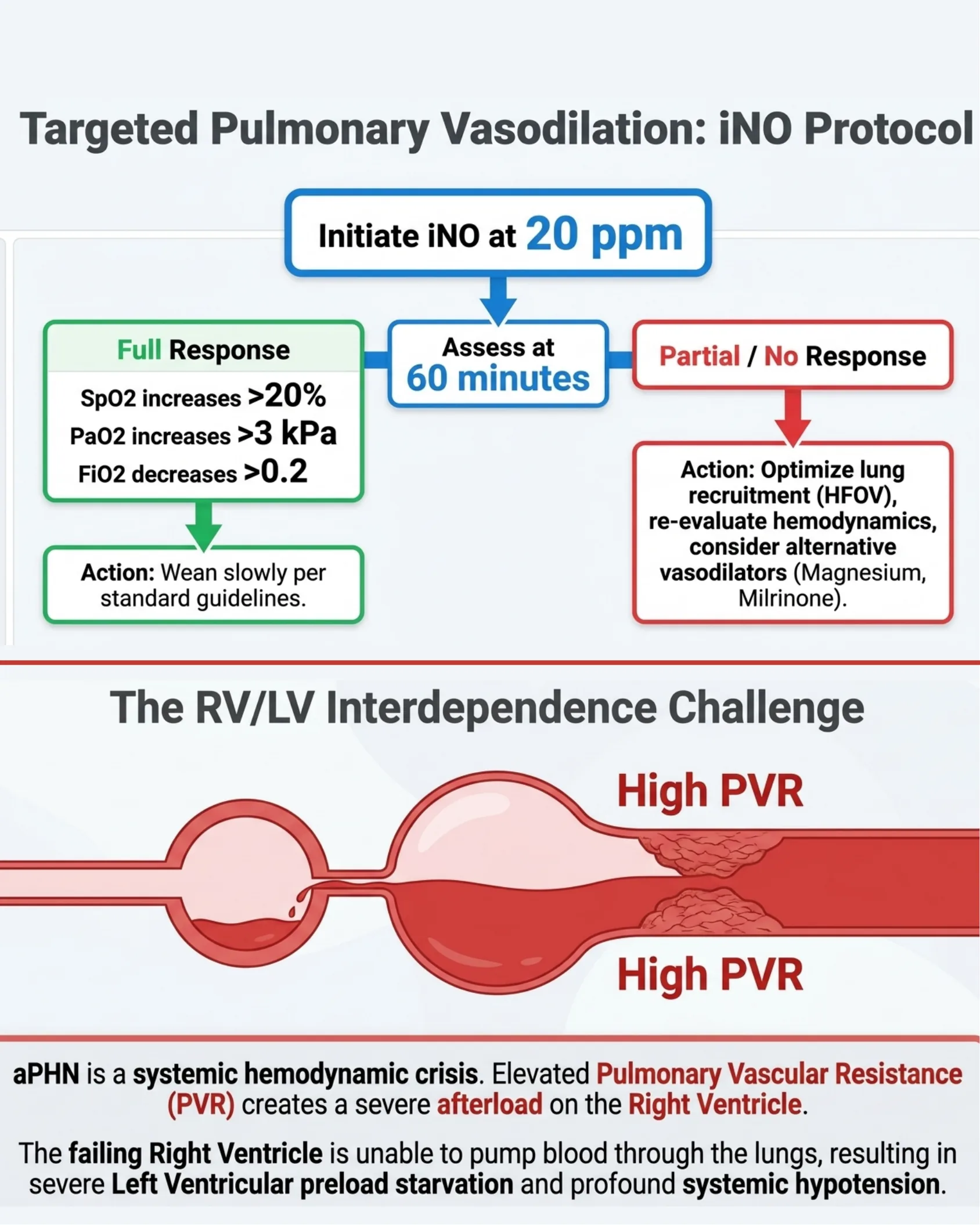
- Initiate iNO at 20 ppm
- Assess at 60 minutes
Full Response:
- SpO2 increases >20%
- PaO2 increases >3 kPa
- FiO2 decreases >0.2
Action: Wean slowly per standard guidelines.
Partial / No Response:
Action: Optimize lung recruitment (HFOV), re-evaluate hemodynamics, consider alternative vasodilators (Magnesium, Milrinone).
The RV/LV Interdependence Challenge
High PVR (Right Ventricle) — High PVR (Left Ventricle pathway)
aPHN is a systemic hemodynamic crisis. Elevated Pulmonary Vascular Resistance (PVR) creates a severe afterload on the Right Ventricle.
The failing Right Ventricle is unable to pump blood through the lungs, resulting in severe Left Ventricular preload starvation and profound systemic hypotension.
Echo-Guided Inotrope Selection Matrix
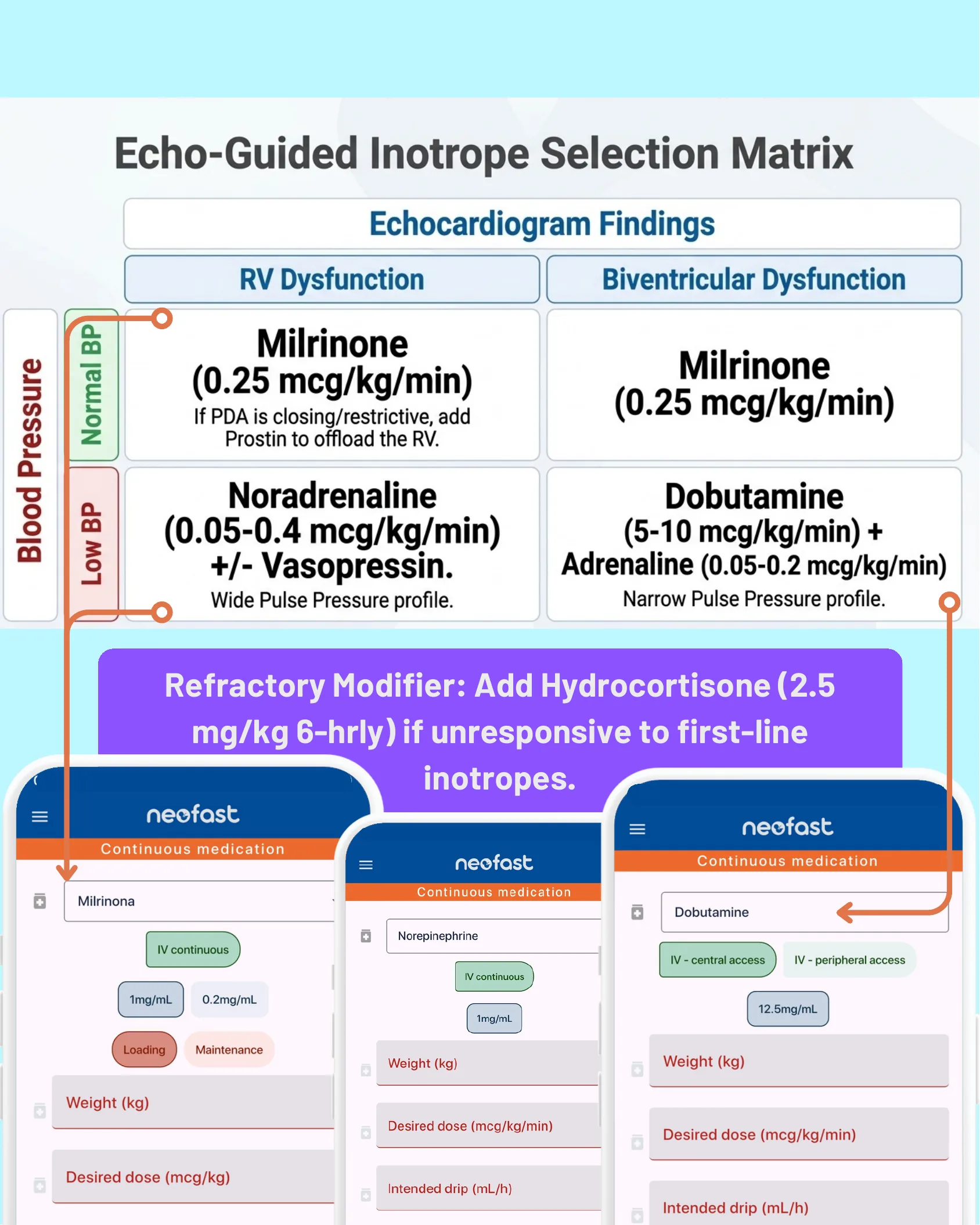
Echo-Guided Inotrope Selection Matrix
| Blood Pressure | RV Dysfunction | Biventricular Dysfunction |
|---|---|---|
| Normal BP | Milrinone (0.25 mcg/kg/min) If PDA is closing/restrictive, add Prostin to offload the RV. | Milrinone (0.25 mcg/kg/min) |
| Low BP | Noradrenaline (0.05-0.4 mcg/kg/min) +/- Vasopressin. Wide Pulse Pressure profile. | Dobutamine (5-10 mcg/kg/min) + Adrenaline (0.05-0.2 mcg/kg/min) Narrow Pulse Pressure profile. |
Refractory Modifier: Add Hydrocortisone (2.5 mg/kg 6-hrly) if unresponsive to first-line inotropes.
- NeoFast App Screenshot 1: Continuous medication – Milrinona, IV continuous, concentrations 1mg/mL or 0.2mg/mL, options for Loading or Maintenance, fields for Weight (kg) and Desired dose (mcg/kg).
- NeoFast App Screenshot 2: Continuous medication – Norepinephrine, IV continuous, concentration 1mg/mL, fields for Weight (kg), Desired dose (mcg/kg/min), Intended drip (mL/h).
- NeoFast App Screenshot 3: Continuous medication – Dobutamine, IV – central access or IV – peripheral access, concentration 12.5mg/mL, fields for Weight (kg), Desired dose (mcg/kg/min), Intended drip (mL/h).
Refractory aPHN: ECLS (ECMO) Criteria
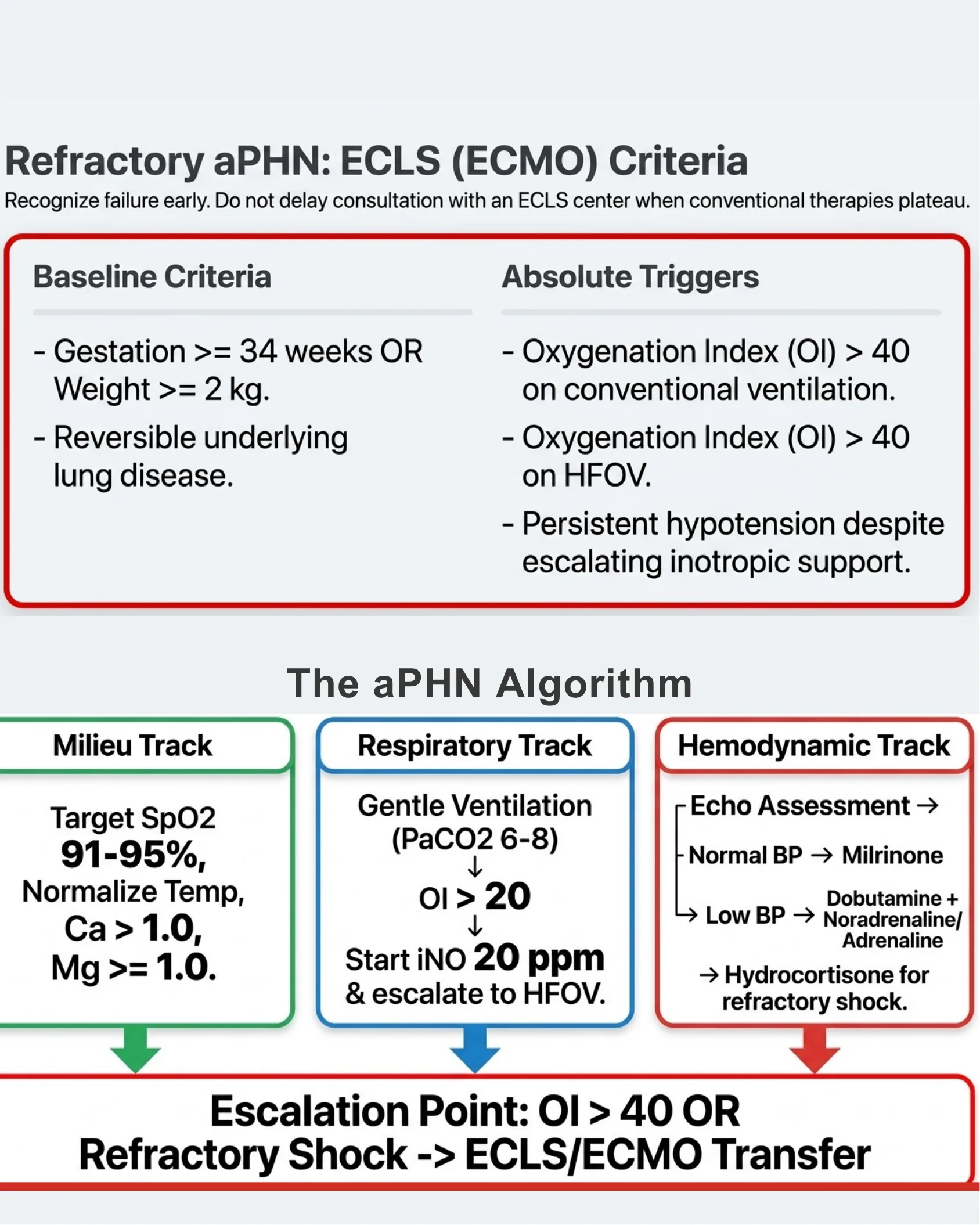
Refractory aPHN: ECLS (ECMO) Criteria
Recognize failure early. Do not delay consultation with an ECLS center when conventional therapies plateau.
Baseline Criteria
- Gestation >= 34 weeks OR Weight >= 2 kg.
- Reversible underlying lung disease.
Absolute Triggers
- Oxygenation Index (OI) > 40 on conventional ventilation.
- Oxygenation Index (OI) > 40 on HFOV.
- Persistent hypotension despite escalating inotropic support.
The aPHN Algorithm
| Milieu Track | Respiratory Track | Hemodynamic Track |
|---|---|---|
| Target SpO2 91-95%, Normalize Temp, Ca > 1.0, Mg >= 1.0. | Gentle Ventilation (PaCO2 6-8) → OI > 20 → Start iNO 20 ppm & escalate to HFOV. | Echo Assessment → Normal BP → Milrinone → Low BP → Dobutamine + Noradrenaline/Adrenaline → Hydrocortisone for refractory shock. |
Escalation Point: OI > 40 OR Refractory Shock -> ECLS/ECMO Transfer
NeoFast App Overview

NeoFast App Main Menu
The NeoFast app provides a suite of neonatal clinical calculation tools, available in multiple languages as represented by the globe of international flags.
- Venous hydration
- Continuous medication
- Medicines
- Intubation
- Other calculations
- (Tools/procedures icon)