
Interactive dosing calculations shown below are from the NeoFast app.
Bedside Clinical Guidelines Partnership and the NHS network of West Midlands.
Precision Management of Early-Onset Sepsis — A phenotype-driven approach to antibiotic eradication and hemodynamic rescue in the neonate.
A Unified Protocol
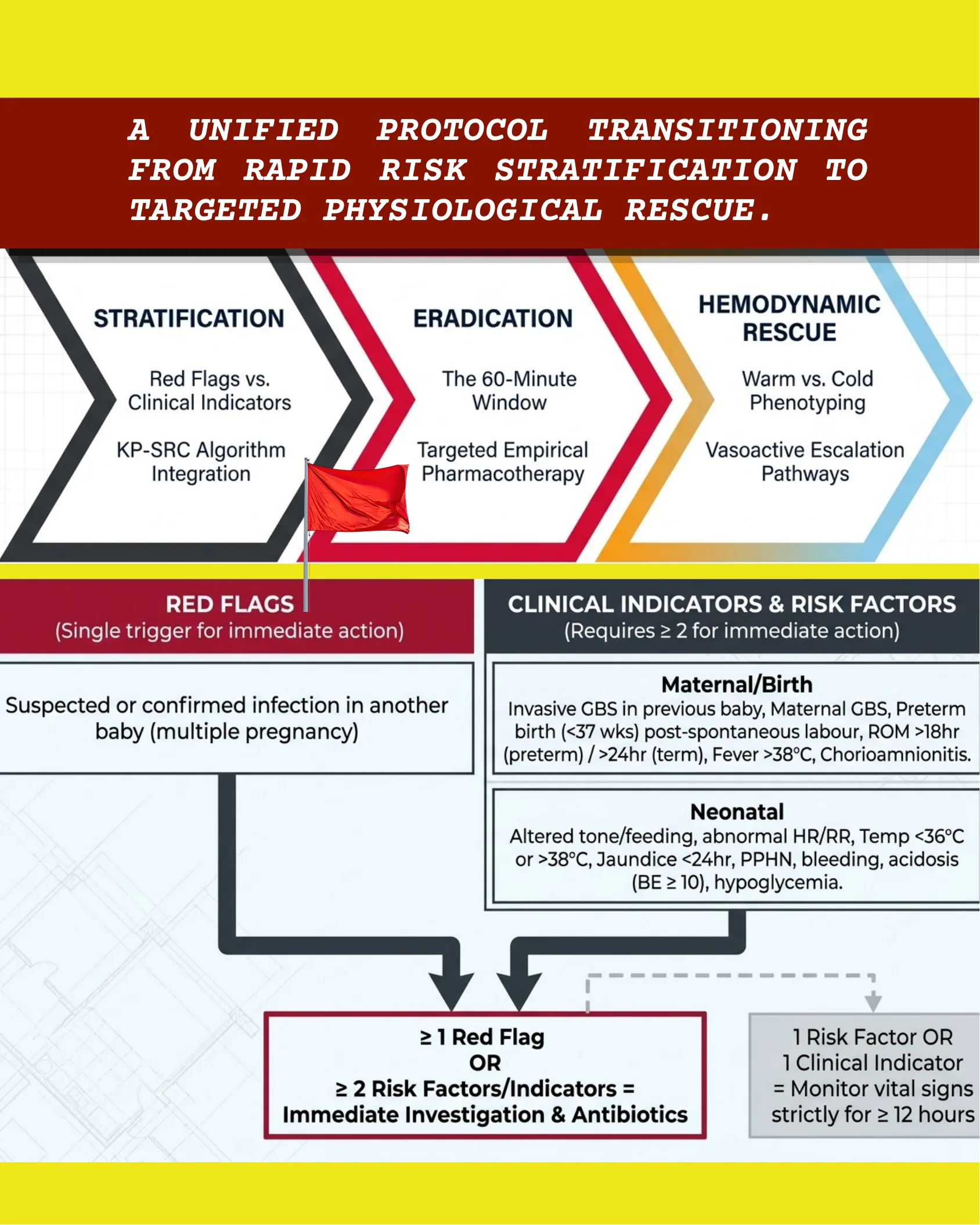
A unified protocol transitioning from rapid risk stratification to targeted physiological rescue.
Three stages:
- Stratification — Red Flags vs. Clinical Indicators; KP-SRC algorithm integration.
- Eradication — The 60-minute window; targeted empirical pharmacotherapy.
- Hemodynamic Rescue — Warm vs. Cold phenotyping; vasoactive escalation pathways.
Red Flags (single trigger for immediate action)
Suspected or confirmed infection in another baby (multiple pregnancy).
Clinical Indicators & Risk Factors (requires ≥ 2 for immediate action)
Maternal/Birth: Invasive GBS in previous baby, maternal GBS, preterm birth (<37 wks) post-spontaneous labour, ROM >18 hr (preterm) / >24 hr (term), fever >38 °C, chorioamnionitis.
Neonatal: Altered tone/feeding, abnormal HR/RR, temp <36 °C or >38 °C, jaundice <24 hr, PPHN, bleeding, acidosis (BE ≥ 10), hypoglycemia.
Decision: ≥ 1 Red Flag OR ≥ 2 Risk Factors/Indicators = immediate investigation & antibiotics. 1 Risk Factor OR 1 Clinical Indicator = monitor vital signs strictly for ≥ 12 hours.
Candidate Identification (KP-SRC)
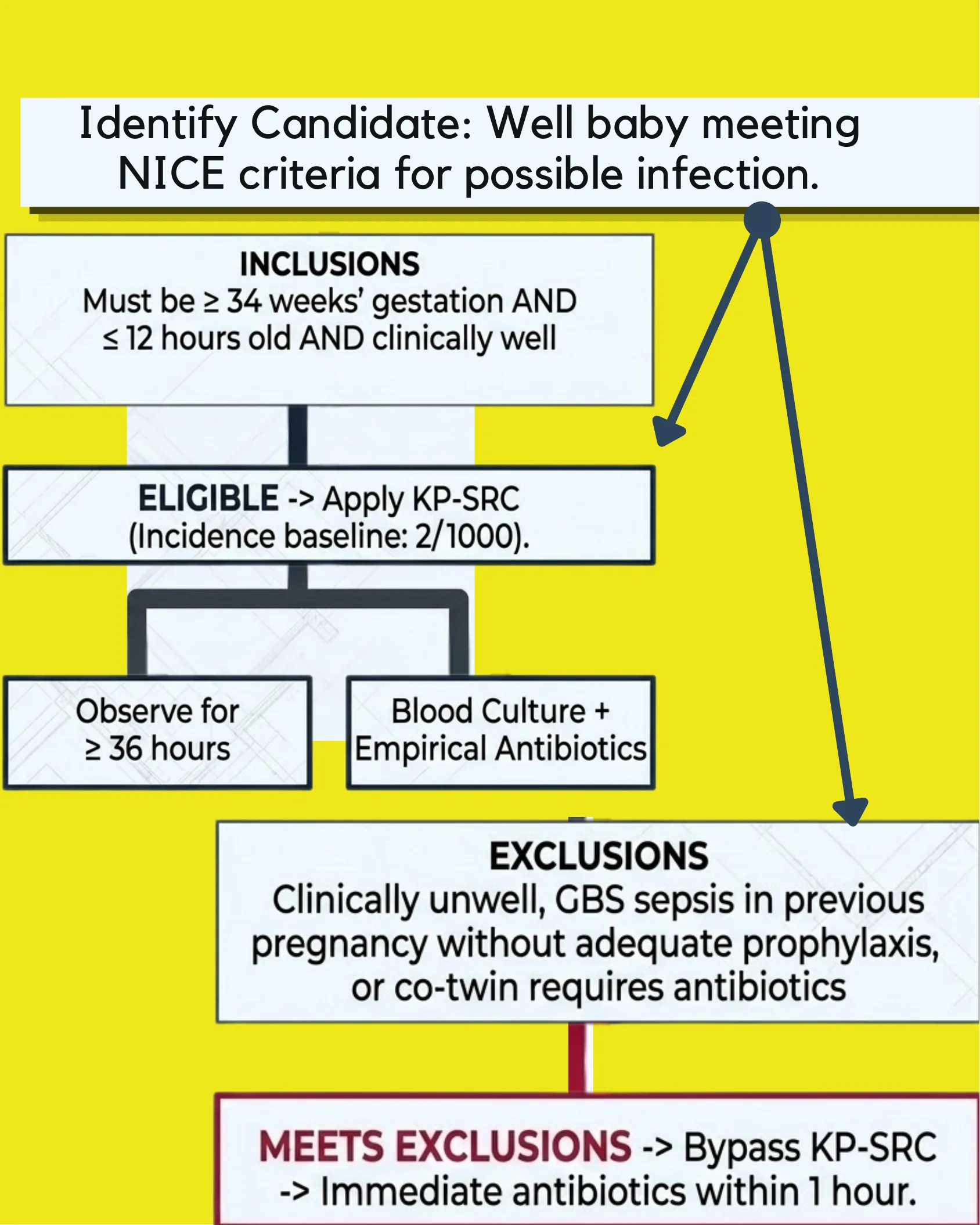
Identify candidate: Well baby meeting NICE criteria for possible infection.
Inclusions: Must be ≥ 34 weeks’ gestation AND ≤ 12 hours old AND clinically well.
Eligible → Apply KP-SRC (incidence baseline: 2/1000). Options: observe for ≥ 36 hours, or blood culture + empirical antibiotics.
Exclusions: Clinically unwell, GBS sepsis in previous pregnancy without adequate prophylaxis, or co-twin requires antibiotics.
Meets exclusions → Bypass KP-SRC → Immediate antibiotics within 1 hour.
The Golden Hour Timeline
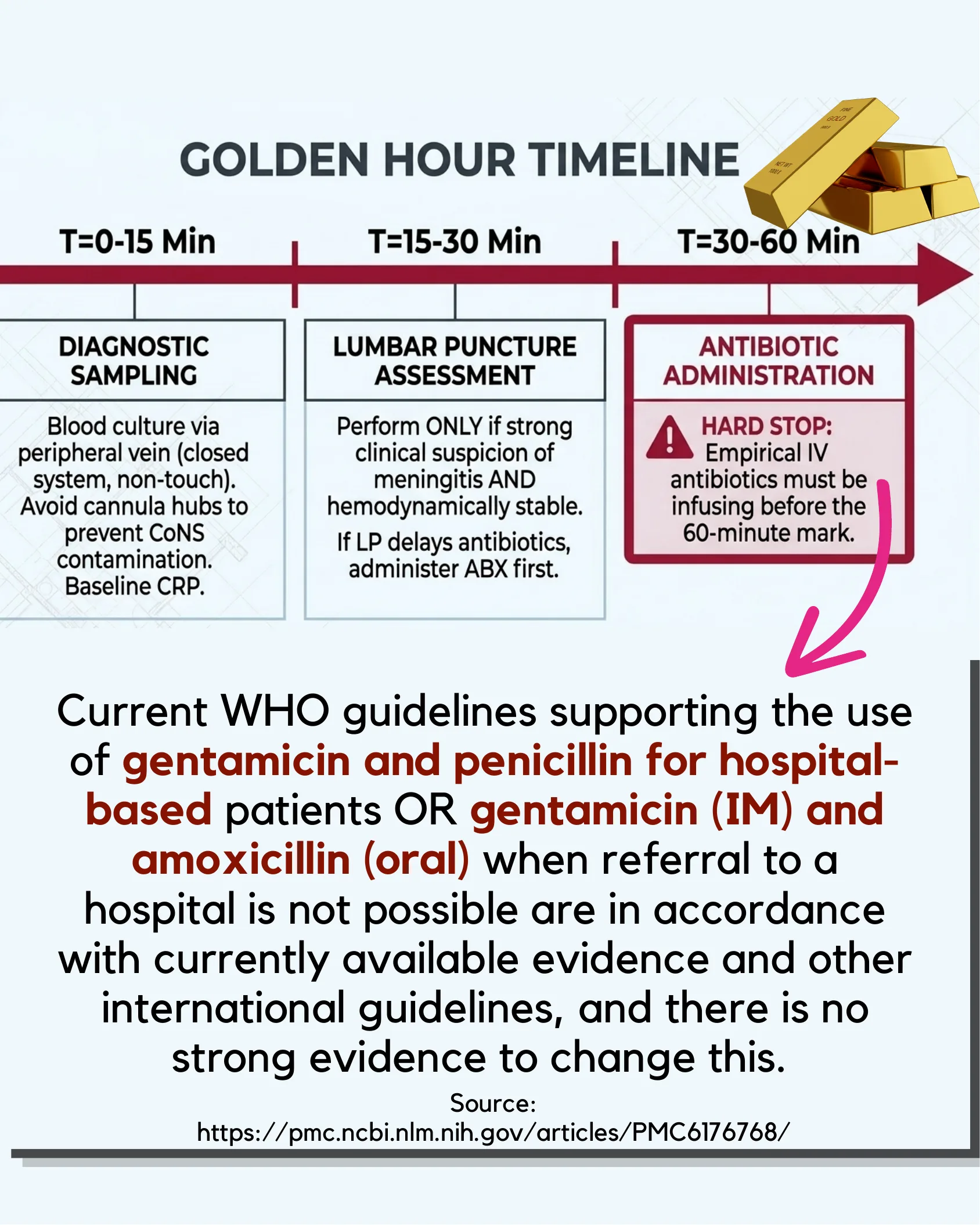
- T = 0–15 min — Diagnostic sampling: Blood culture via peripheral vein (closed system, non-touch). Avoid cannula hubs to prevent CoNS contamination. Baseline CRP.
- T = 15–30 min — Lumbar puncture assessment: Perform ONLY if strong clinical suspicion of meningitis AND hemodynamically stable. If LP delays antibiotics, administer ABX first.
- T = 30–60 min — Antibiotic administration: HARD STOP — Empirical IV antibiotics must be infusing before the 60-minute mark.
Current WHO guidelines supporting the use of gentamicin and penicillin for hospital-based patients OR gentamicin (IM) and amoxicillin (oral) when referral to a hospital is not possible are in accordance with currently available evidence and other international guidelines, and there is no strong evidence to change this.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC6176768/
First-Line Empirical Therapy
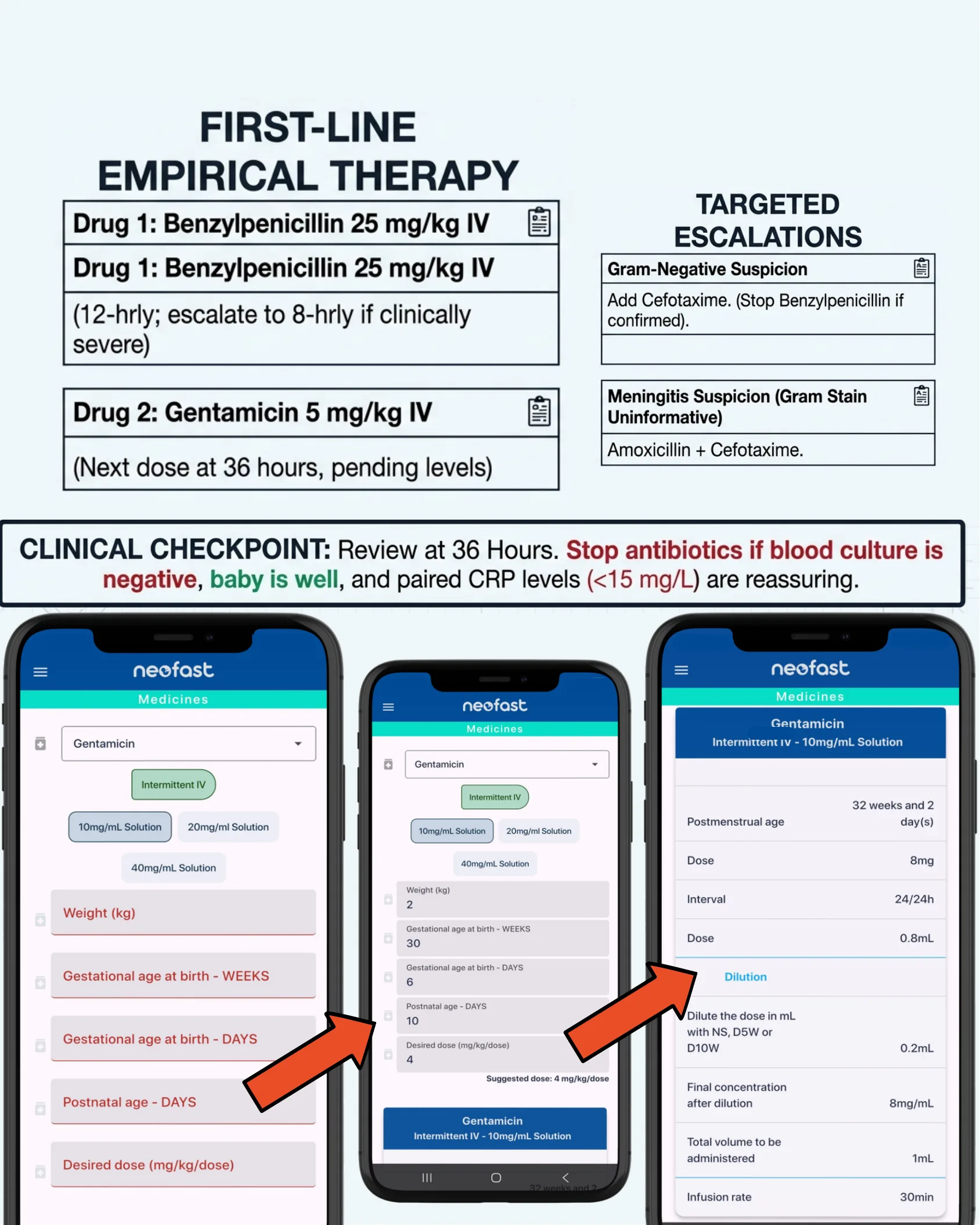
Drug 1: Benzylpenicillin 25 mg/kg IV (12-hrly; escalate to 8-hrly if clinically severe).
Drug 2: Gentamicin 5 mg/kg IV (next dose at 36 hours, pending levels).
Targeted Escalations
- Gram-Negative Suspicion: Add Cefotaxime (stop Benzylpenicillin if confirmed).
- Meningitis Suspicion (Gram stain uninformative): Amoxicillin + Cefotaxime.
Clinical Checkpoint — Review at 36 Hours: Stop antibiotics if blood culture is negative, baby is well, and paired CRP levels (<15 mg/L) are reassuring.
Hemodynamic Phenotyping: Warm vs. Cold Shock
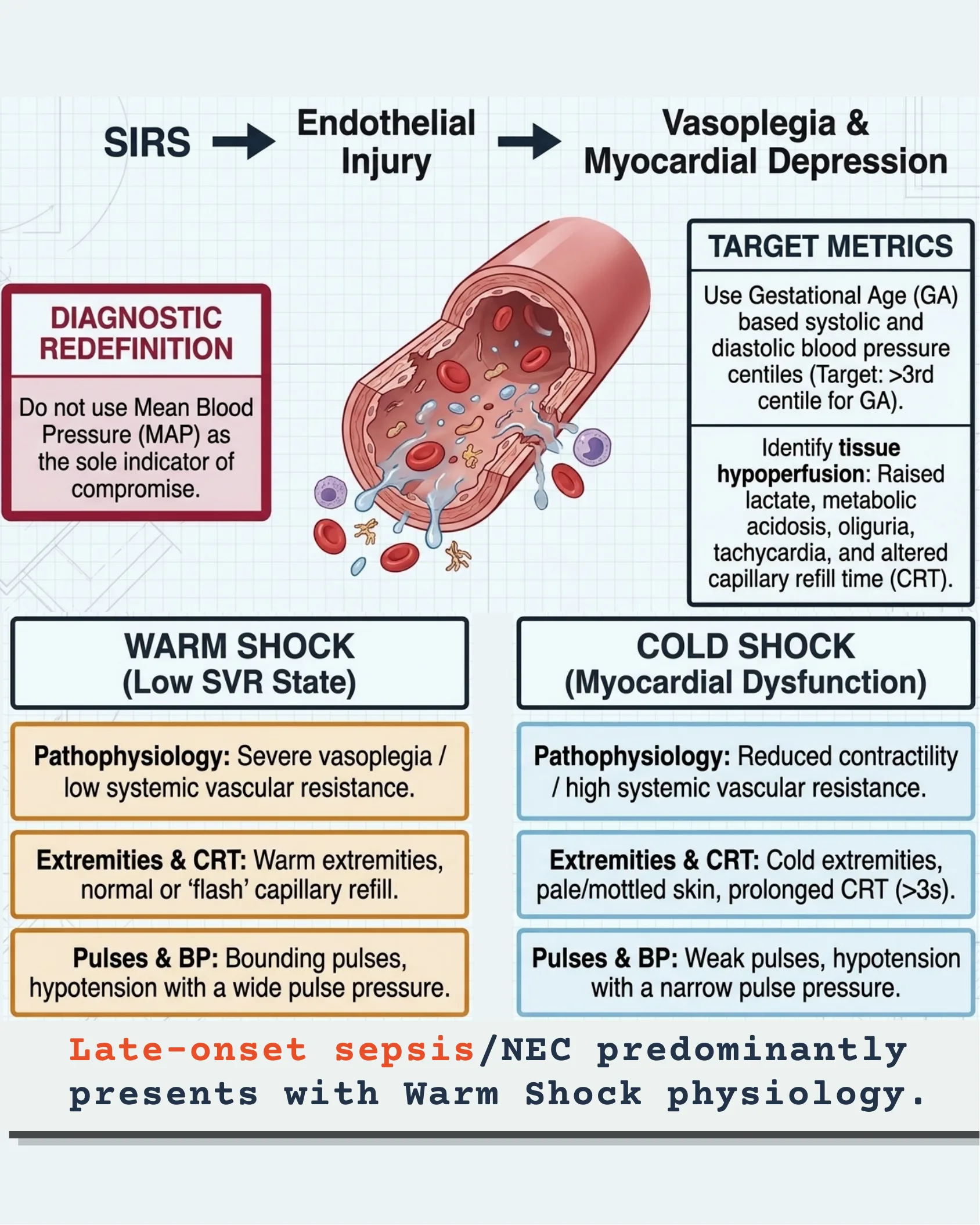
Cascade: SIRS → Endothelial Injury → Vasoplegia & Myocardial Depression.
Diagnostic redefinition: Do not use Mean Blood Pressure (MAP) as the sole indicator of compromise.
Target metrics: Use Gestational Age (GA)-based systolic and diastolic blood pressure centiles (target: >3rd centile for GA). Identify tissue hypoperfusion: raised lactate, metabolic acidosis, oliguria, tachycardia, and altered capillary refill time (CRT).
Warm Shock (Low SVR State)
- Pathophysiology: Severe vasoplegia / low systemic vascular resistance.
- Extremities & CRT: Warm extremities, normal or ‘flash’ capillary refill.
- Pulses & BP: Bounding pulses, hypotension with a wide pulse pressure.
Cold Shock (Myocardial Dysfunction)
- Pathophysiology: Reduced contractility / high systemic vascular resistance.
- Extremities & CRT: Cold extremities, pale/mottled skin, prolonged CRT (>3 s).
- Pulses & BP: Weak pulses, hypotension with a narrow pulse pressure.
Late-onset sepsis/NEC predominantly presents with Warm Shock physiology.
Fluid Resuscitation & Warm Shock Pathway
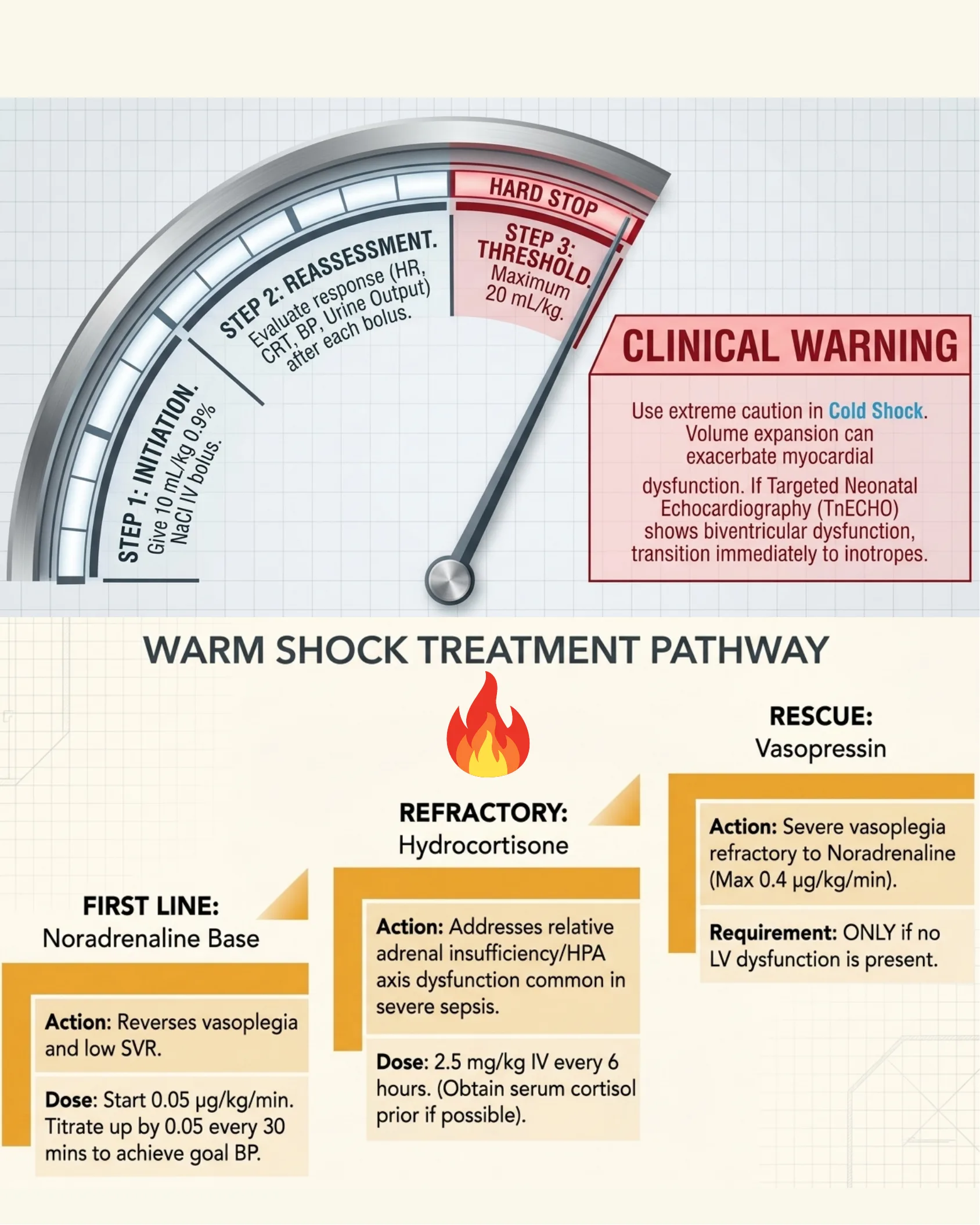
Fluid Resuscitation Gauge
- Step 1 — Initiation: Give 10 mL/kg 0.9% NaCl IV bolus.
- Step 2 — Reassessment: Evaluate response (HR, CRT, BP, urine output) after each bolus.
- Step 3 — Threshold (HARD STOP): Maximum 20 mL/kg.
Clinical warning: Use extreme caution in Cold Shock. Volume expansion can exacerbate myocardial dysfunction. If Targeted Neonatal Echocardiography (TnECHO) shows biventricular dysfunction, transition immediately to inotropes.
Warm Shock Treatment Pathway
- First line — Noradrenaline base. Action: reverses vasoplegia and low SVR. Dose: start 0.05 µg/kg/min. Titrate up by 0.05 every 30 mins to achieve goal BP.
- Refractory — Hydrocortisone. Action: addresses relative adrenal insufficiency/HPA axis dysfunction common in severe sepsis. Dose: 2.5 mg/kg IV every 6 hours (obtain serum cortisol prior if possible).
- Rescue — Vasopressin. Action: severe vasoplegia refractory to Noradrenaline (max 0.4 µg/kg/min). Requirement: ONLY if no LV dysfunction is present.
First Line: Noradrenaline (in the NeoFast app)
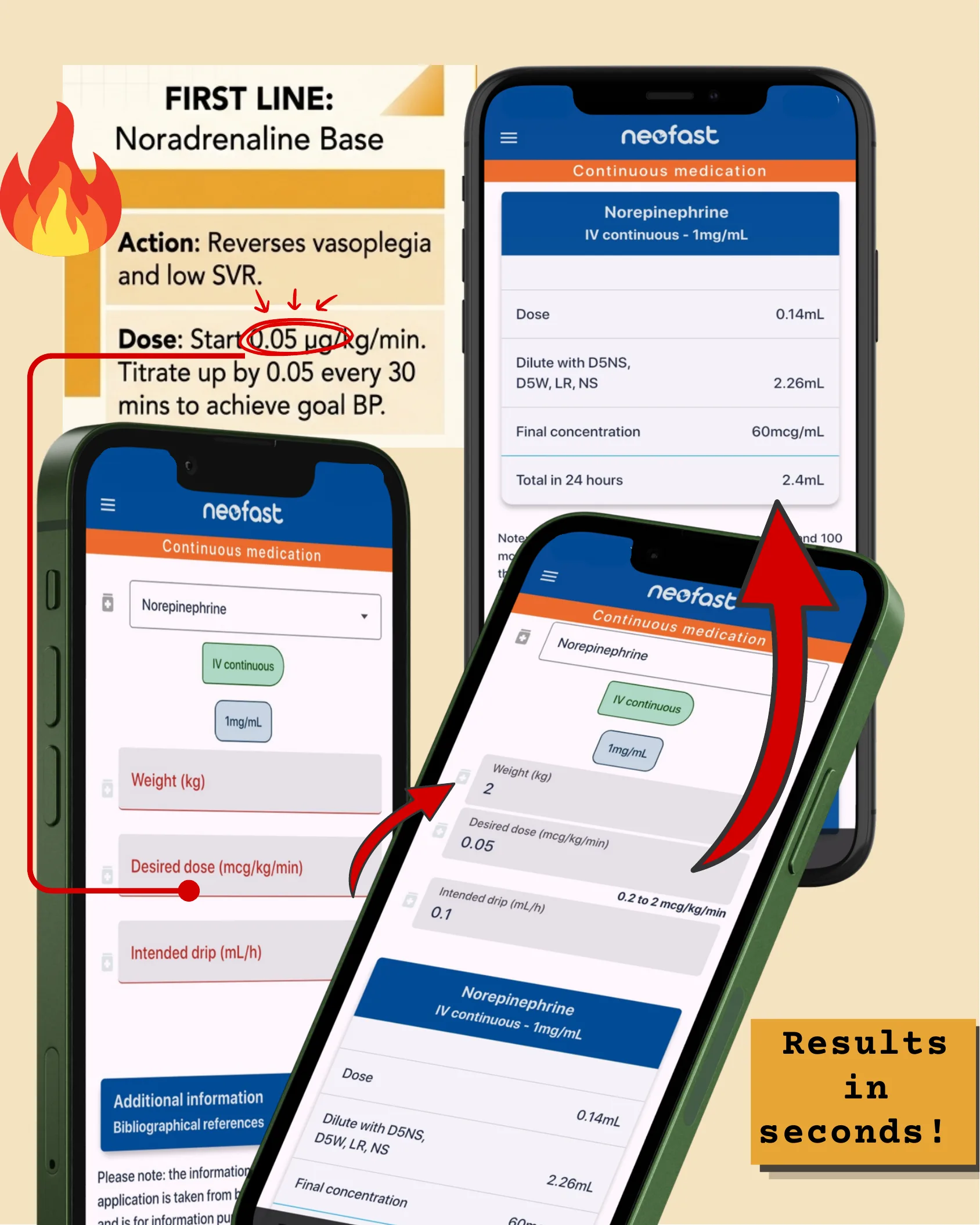
First line — Noradrenaline base. Action: reverses vasoplegia and low SVR. Dose: start 0.05 µg/kg/min; titrate up by 0.05 every 30 mins to achieve goal BP.
NeoFast example (Norepinephrine, IV continuous, 1 mg/mL): desired dose 0.05 mcg/kg/min → dose 0.14 mL; dilute with D5NS, D5W, LR, NS 2.26 mL; final concentration 60 mcg/mL; total in 24 hours 2.4 mL. Results in seconds.
Refractory: Hydrocortisone (in the NeoFast app)
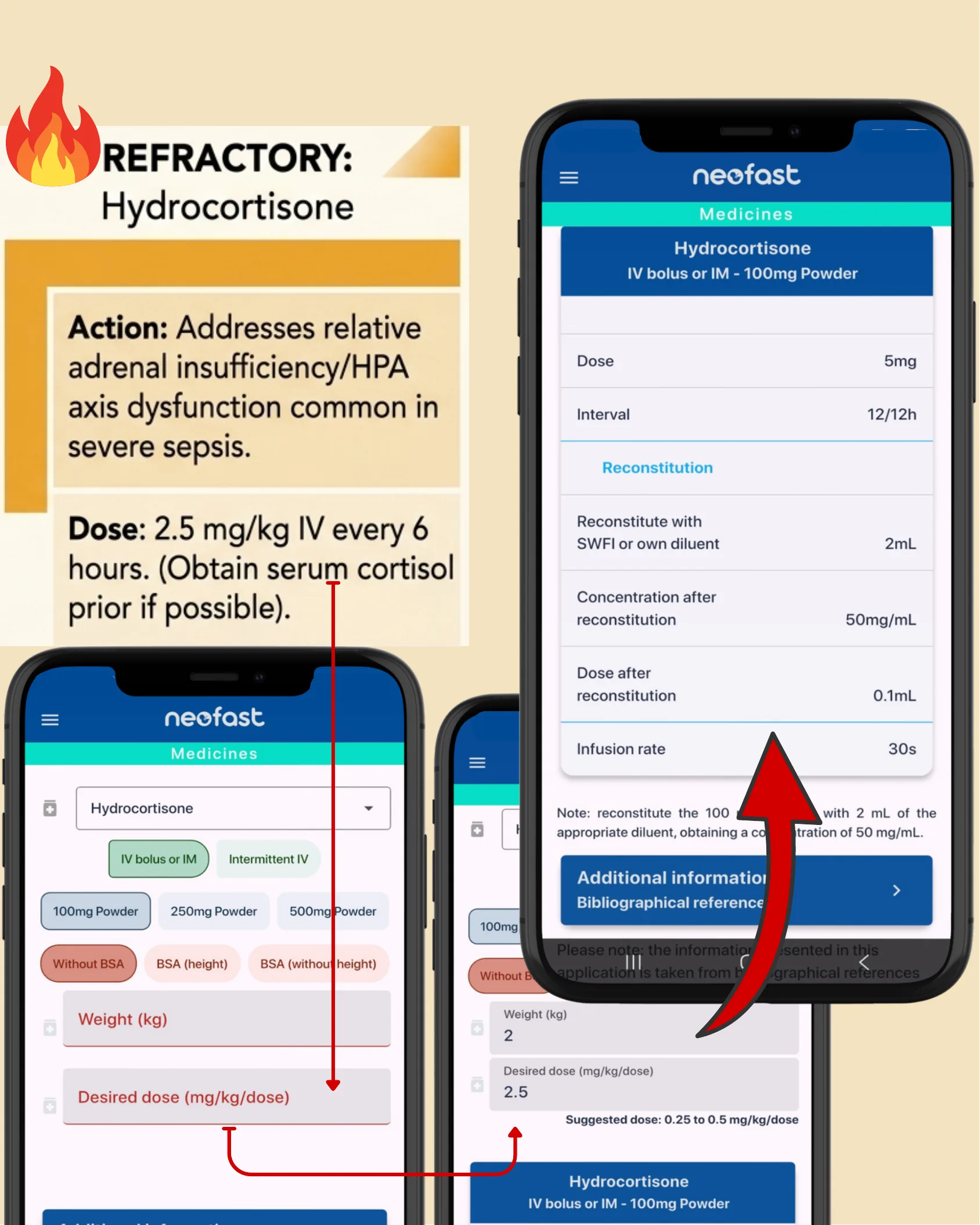
Refractory — Hydrocortisone. Action: addresses relative adrenal insufficiency/HPA axis dysfunction common in severe sepsis. Dose: 2.5 mg/kg IV every 6 hours (obtain serum cortisol prior if possible).
NeoFast example (Hydrocortisone, IV bolus or IM, 100 mg powder): dose 5 mg; interval 12/12 h; reconstitute with SWFI or own diluent 2 mL; concentration after reconstitution 50 mg/mL; dose after reconstitution 0.1 mL; infusion rate 30 s.
Rescue: Vasopressin (in the NeoFast app)
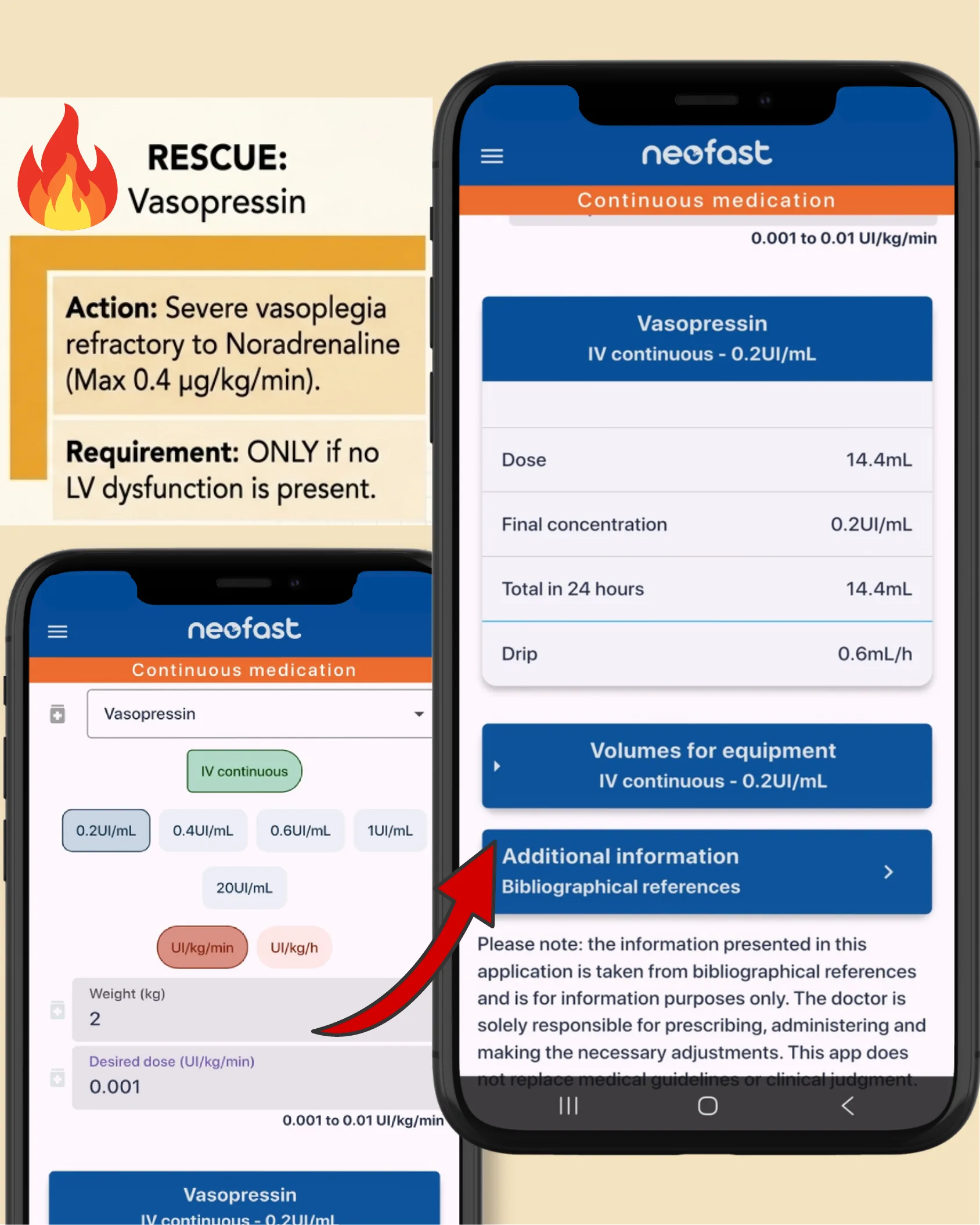
Rescue — Vasopressin. Action: severe vasoplegia refractory to Noradrenaline (max 0.4 µg/kg/min). Requirement: ONLY if no LV dysfunction is present.
NeoFast example (Vasopressin, IV continuous, 0.2 UI/mL): desired dose 0.001 UI/kg/min (range 0.001 to 0.01); dose 14.4 mL; final concentration 0.2 UI/mL; total in 24 hours 14.4 mL; drip 0.6 mL/h.
Note: the information presented in this application is taken from bibliographical references and is for information purposes only. The doctor is solely responsible for prescribing, administering and making the necessary adjustments. This app does not replace medical guidelines or clinical judgment.
Cold Shock Treatment Pathway
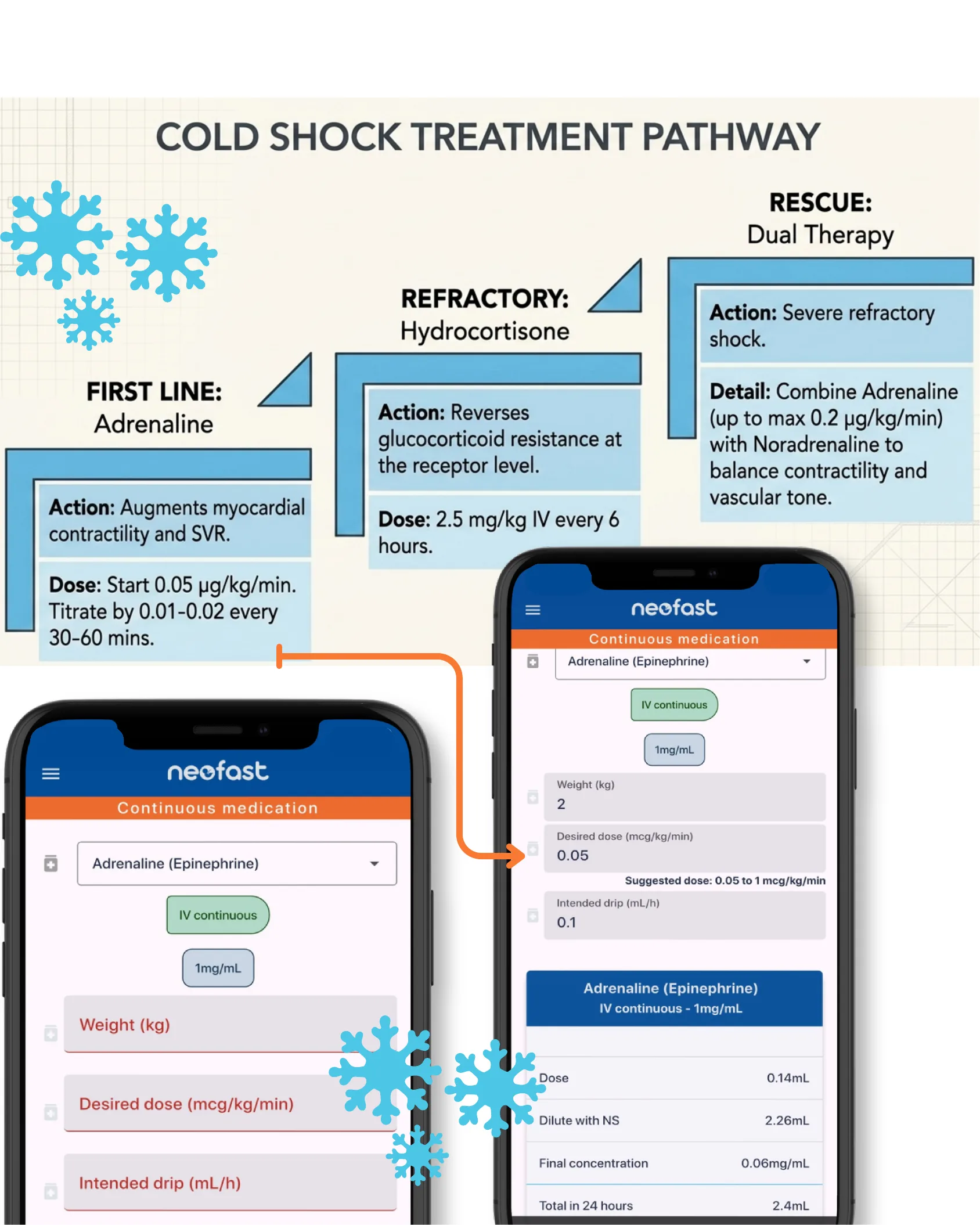
- First line — Adrenaline. Action: augments myocardial contractility and SVR. Dose: start 0.05 µg/kg/min. Titrate by 0.01–0.02 every 30–60 mins.
- Refractory — Hydrocortisone. Action: reverses glucocorticoid resistance at the receptor level. Dose: 2.5 mg/kg IV every 6 hours.
- Rescue — Dual Therapy. Action: severe refractory shock. Detail: combine Adrenaline (up to max 0.2 µg/kg/min) with Noradrenaline to balance contractility and vascular tone.
NeoFast example (Adrenaline/Epinephrine, IV continuous, 1 mg/mL): desired dose 0.05 mcg/kg/min (suggested 0.05 to 1); dose 0.14 mL; dilute with NS 2.26 mL; final concentration 0.06 mg/mL; total in 24 hours 2.4 mL.
Rescue: Dual Therapy (in the NeoFast app)
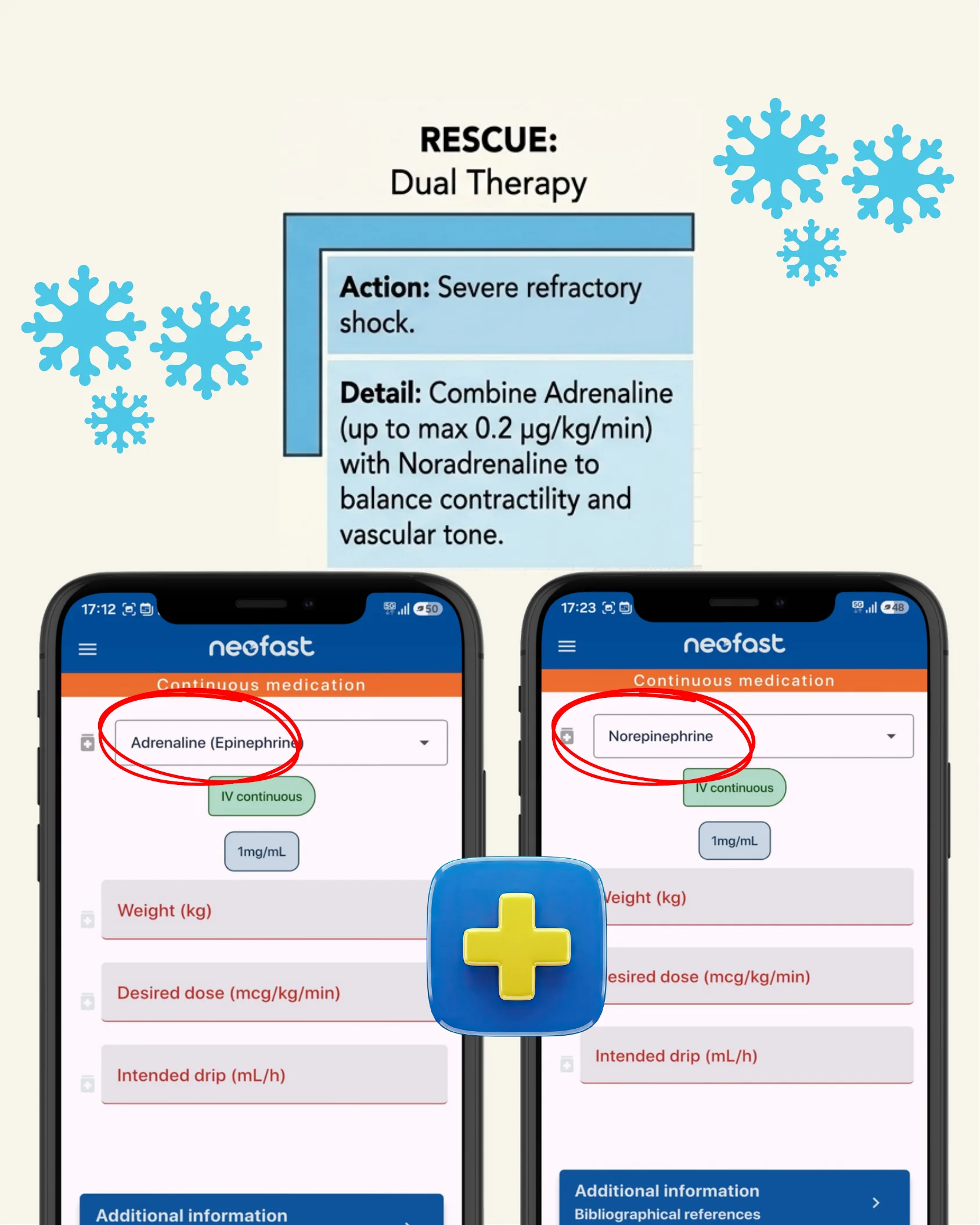
Rescue — Dual Therapy. Action: severe refractory shock. Detail: combine Adrenaline (up to max 0.2 µg/kg/min) with Noradrenaline to balance contractility and vascular tone.
NeoFast lets you calculate both agents side by side — Adrenaline (Epinephrine) and Norepinephrine — for continuous IV infusion.
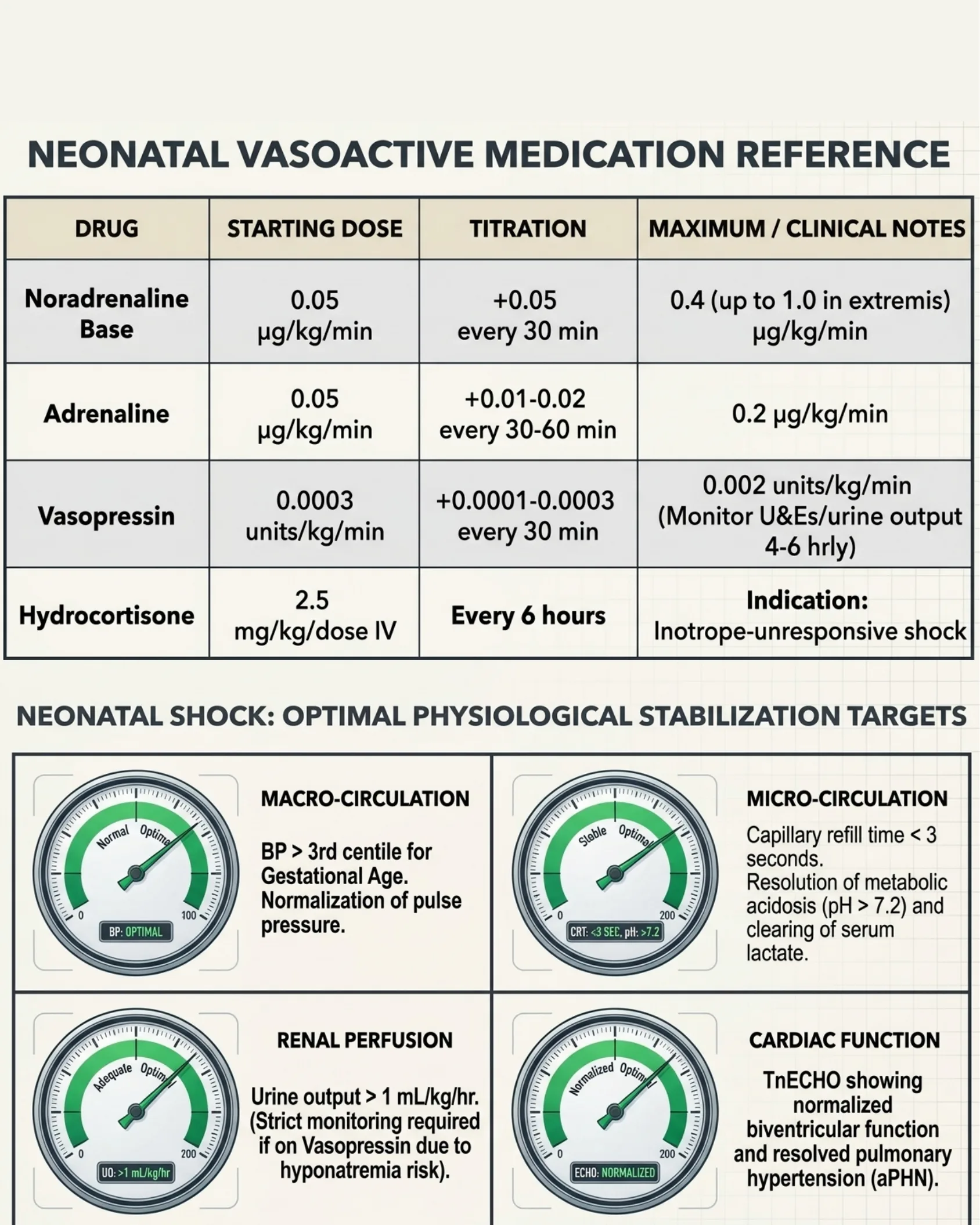
Neonatal Vasoactive Medication Reference
| Drug | Starting dose | Titration | Maximum / Clinical notes |
|---|---|---|---|
| Noradrenaline Base | 0.05 µg/kg/min | +0.05 every 30 min | 0.4 (up to 1.0 in extremis) µg/kg/min |
| Adrenaline | 0.05 µg/kg/min | +0.01–0.02 every 30–60 min | 0.2 µg/kg/min |
| Vasopressin | 0.0003 units/kg/min | +0.0001–0.0003 every 30 min | 0.002 units/kg/min (monitor U&Es/urine output 4–6 hrly) |
| Hydrocortisone | 2.5 mg/kg/dose IV | Every 6 hours | Indication: inotrope-unresponsive shock |
Optimal Physiological Stabilization Targets
- Macro-circulation: BP > 3rd centile for Gestational Age. Normalization of pulse pressure.
- Micro-circulation: Capillary refill time < 3 seconds. Resolution of metabolic acidosis (pH > 7.2) and clearing of serum lactate.
- Renal perfusion: Urine output > 1 mL/kg/hr. (Strict monitoring required if on Vasopressin due to hyponatremia risk.)
- Cardiac function: TnECHO showing normalized biventricular function and resolved pulmonary hypertension (aPHN).
The Cycle at a Glance
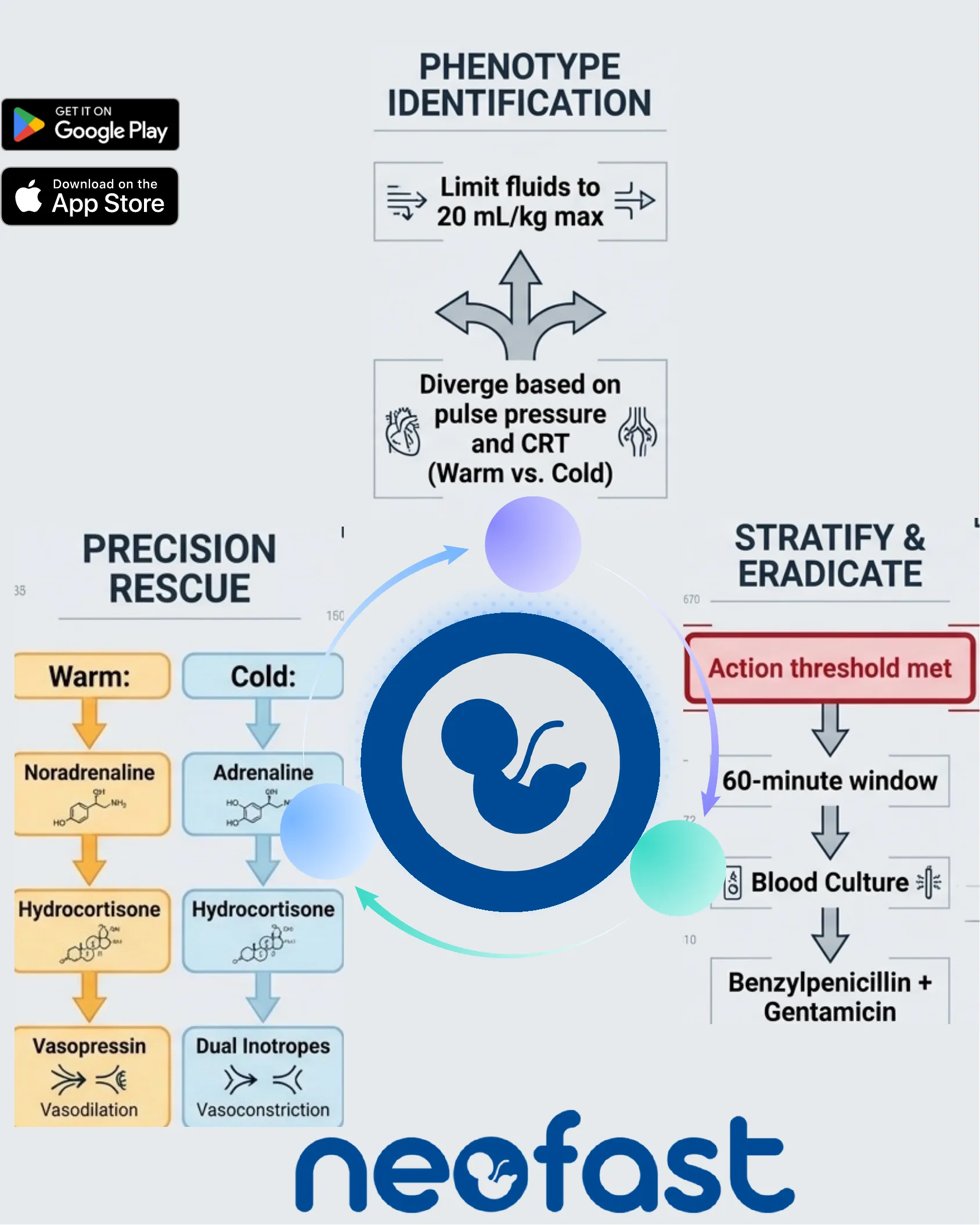
- Phenotype Identification: Limit fluids to 20 mL/kg max; diverge based on pulse pressure and CRT (Warm vs. Cold).
- Stratify & Eradicate: Action threshold met → 60-minute window → Blood Culture → Benzylpenicillin + Gentamicin.
- Precision Rescue — Warm: Noradrenaline → Hydrocortisone → Vasopressin (vasodilation).
- Precision Rescue — Cold: Adrenaline → Hydrocortisone → Dual Inotropes (vasoconstriction).
NeoFast — available on Google Play and the App Store.