
Precision in Neonatal Umbilical Access
Precision in Neonatal Umbilical Access
Evidence-based protocols, exact radiological targeting, and integration with the NeoFast application
Diagnostic Synthesis: Choosing the Right Line
Diagnostic Synthesis: Choosing the Right Line
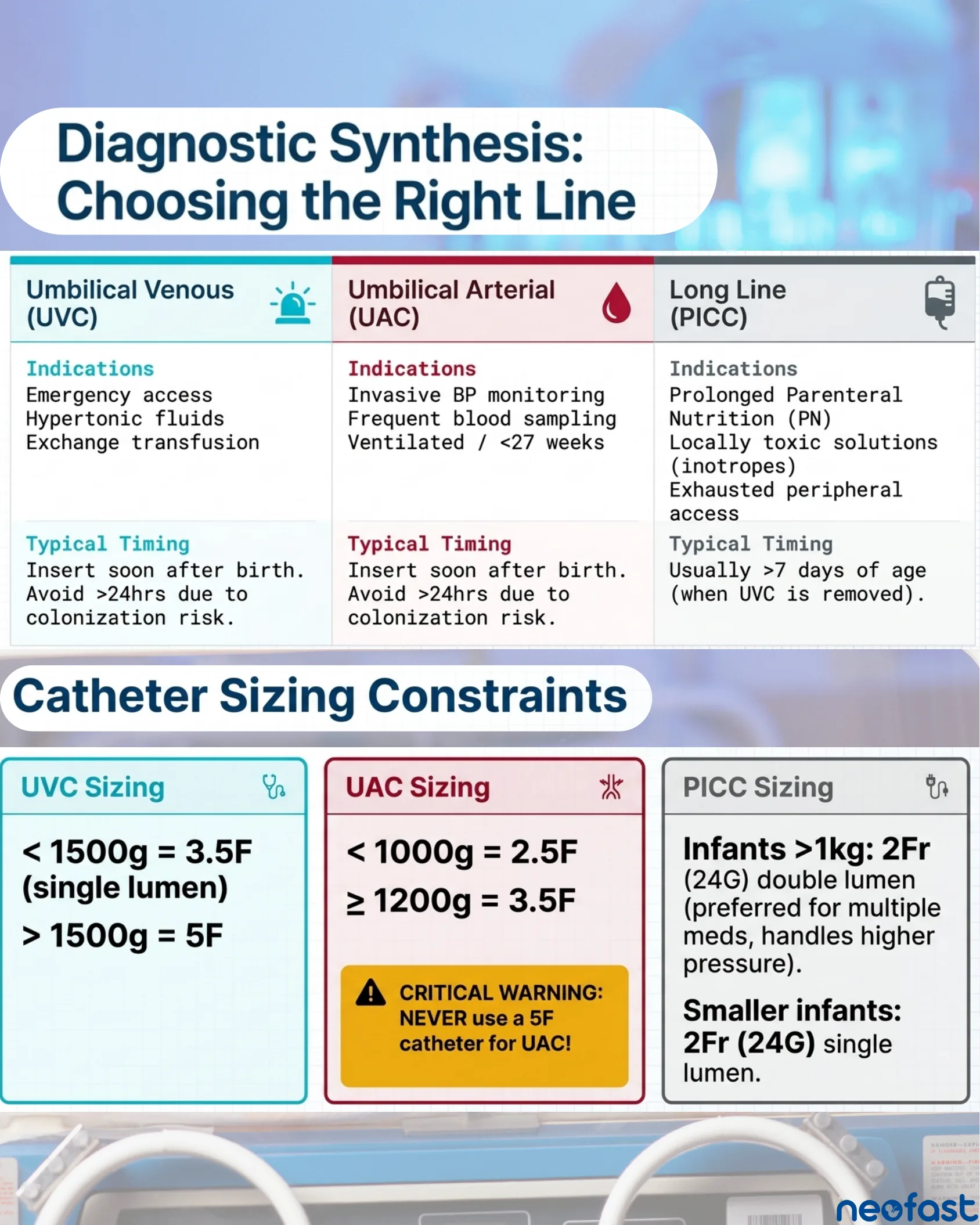
| Umbilical Venous (UVC) | Umbilical Arterial (UAC) | Long Line (PICC) |
|---|---|---|
Indications
| Indications
| Indications
|
| Typical Timing Insert soon after birth. Avoid >24hrs due to colonization risk. | Typical Timing Insert soon after birth. Avoid >24hrs due to colonization risk. | Typical Timing Usually >7 days of age (when UVC is removed). |
Catheter Sizing Constraints
| UVC Sizing | UAC Sizing | PICC Sizing |
|---|---|---|
| < 1500g = 3.5F (single lumen) > 1500g = 5F | < 1000g = 2.5F ≥ 1200g = 3.5F CRITICAL WARNING: NEVER use a 5F catheter for UAC! | Infants >1kg: 2Fr (24G) double lumen (preferred for multiple meds, handles higher pressure). Smaller infants: 2Fr (24G) single lumen. |
Aseptic Foundation & Navigating the Stump
Aseptic Foundation & Navigating the Stump
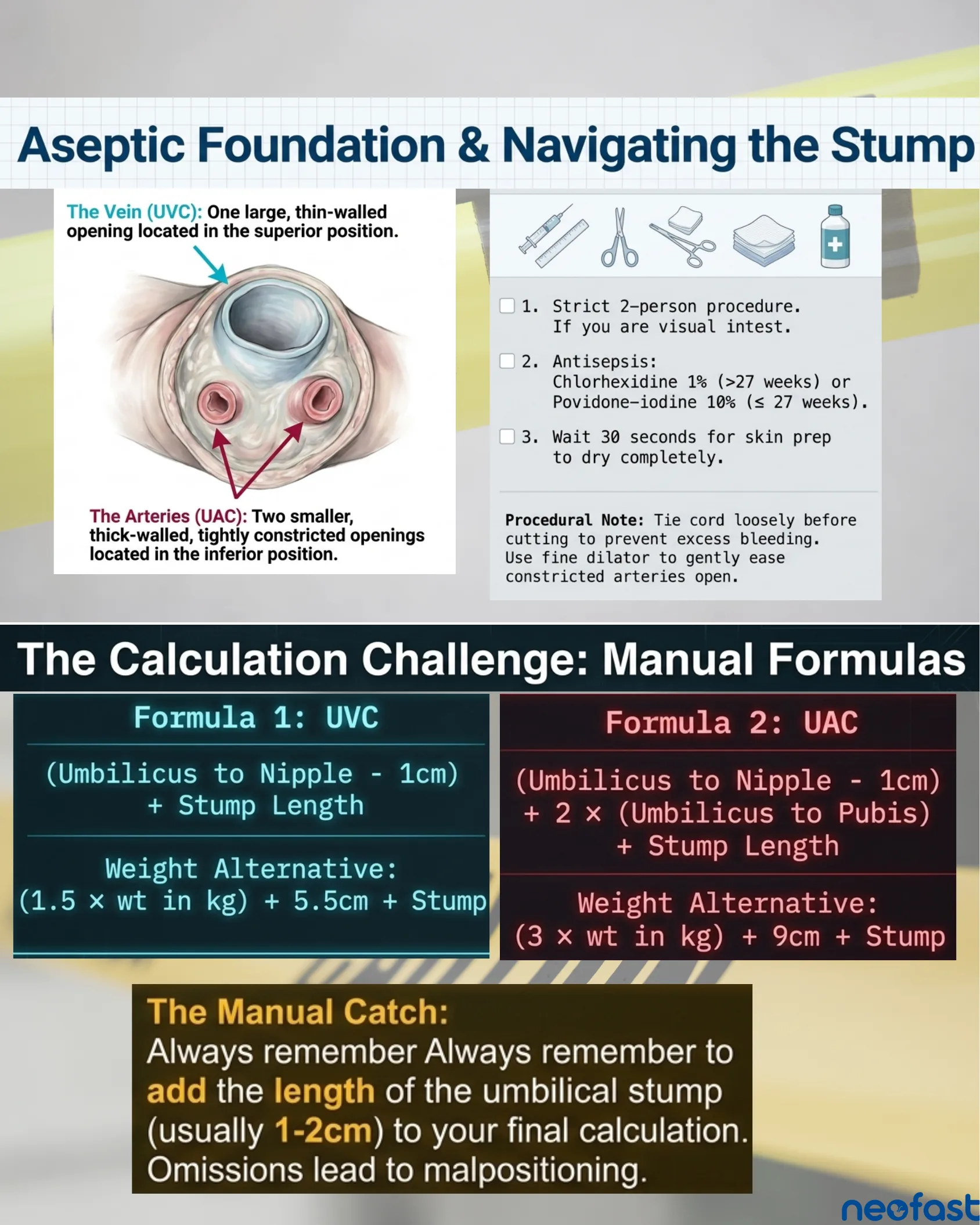
The Vein (UVC): One large, thin-walled opening located in the superior position.
The Arteries (UAC): Two smaller, thick-walled, tightly constricted openings located in the inferior position.
- 1. Strict 2-person procedure. If you are visual in test.
- 2. Antisepsis: Chlorhexidine 1% (>27 weeks) or Povidone-iodine 10% (≤27 weeks).
- 3. Wait 30 seconds for skin prep to dry completely.
Procedural Note: Tie cord loosely before cutting to prevent excess bleeding. Use fine dilator to gently ease constricted arteries open.
The Calculation Challenge: Manual Formulas
| Formula 1: UVC | Formula 2: UAC |
|---|---|
| (Umbilicus to Nipple – 1cm) + Stump Length Weight Alternative: (1.5 × wt in kg) + 5.5cm + Stump | (Umbilicus to Nipple – 1cm) + 2 × (Umbilicus to Pubis) + Stump Length Weight Alternative: (3 × wt in kg) + 9cm + Stump |
The Manual Catch: Always remember to add the length of the umbilical stump (usually 1-2cm) to your final calculation. Omissions lead to malpositioning.
Streamlining Calculations with NeoFast
Streamlining Calculations with NeoFast
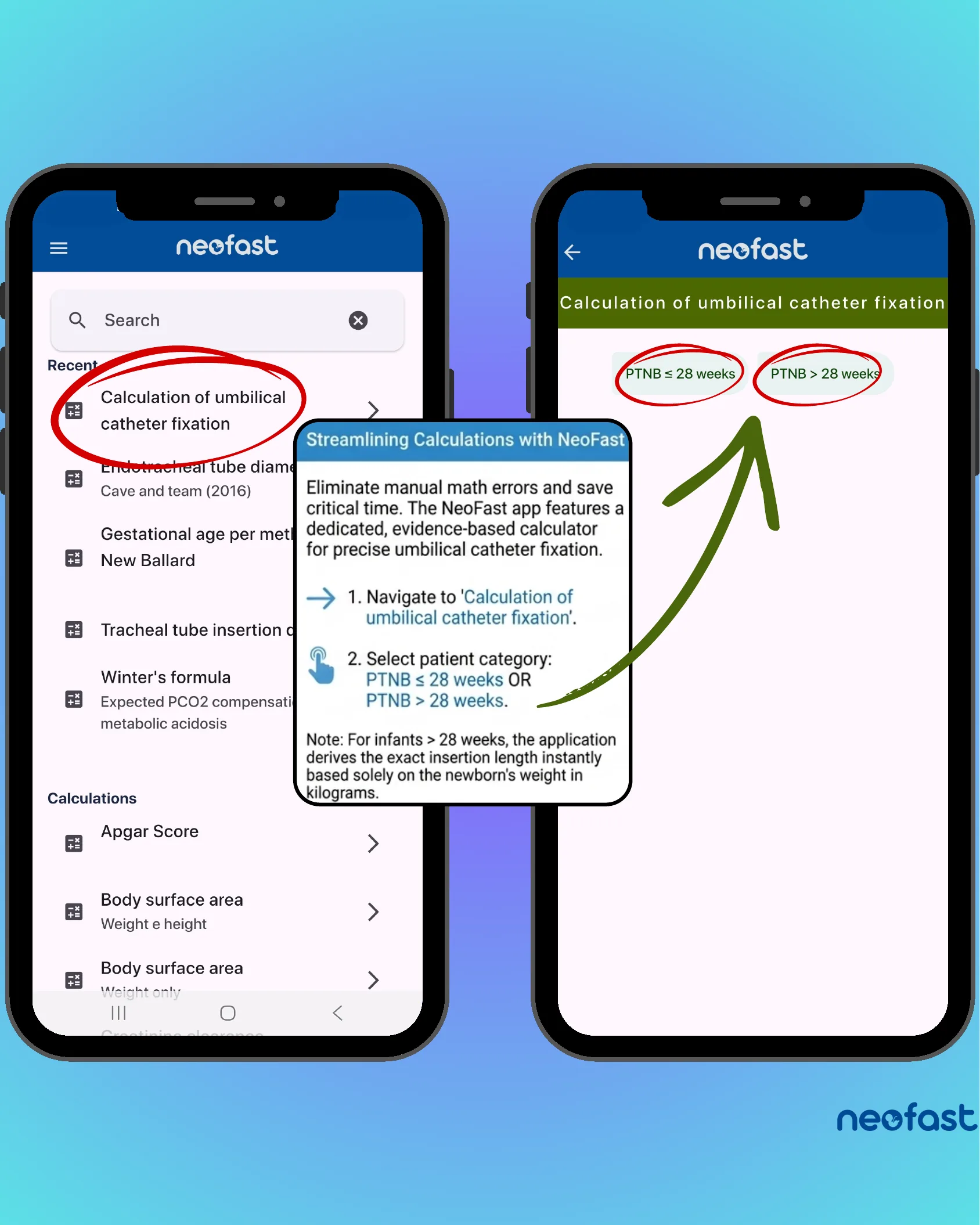
Eliminate manual math errors and save critical time. The NeoFast app features a dedicated, evidence-based calculator for precise umbilical catheter fixation.
- 1. Navigate to ‘Calculation of umbilical catheter fixation’.
- 2. Select patient category: PTNB ≤ 28 weeks OR PTNB > 28 weeks.
Note: For infants > 28 weeks, the application derives the exact insertion length instantly based solely on the newborn’s weight in kilograms.
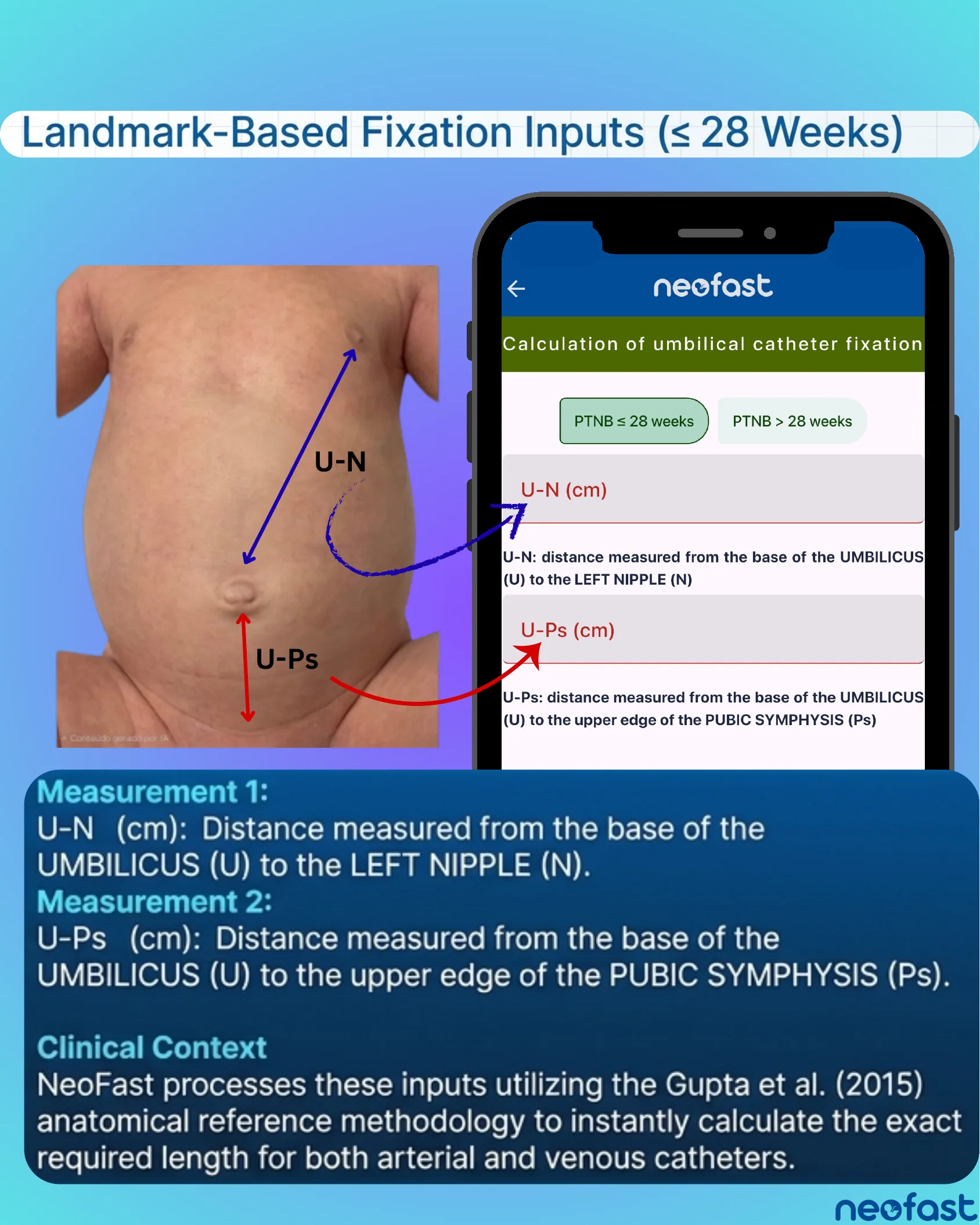
Landmark-Based Fixation Inputs (≤ 28 Weeks)
Landmark-Based Fixation Inputs (≤ 28 Weeks)
Measurement 1:
U-N (cm): Distance measured from the base of the UMBILICUS (U) to the LEFT NIPPLE (N).
Measurement 2:
U-Ps (cm): Distance measured from the base of the UMBILICUS (U) to the upper edge of the PUBIC SYMPHYSIS (Ps).
Clinical Context
NeoFast processes these inputs utilizing the Gupta et al. (2015) anatomical reference methodology to instantly calculate the exact required length for both arterial and venous catheters.
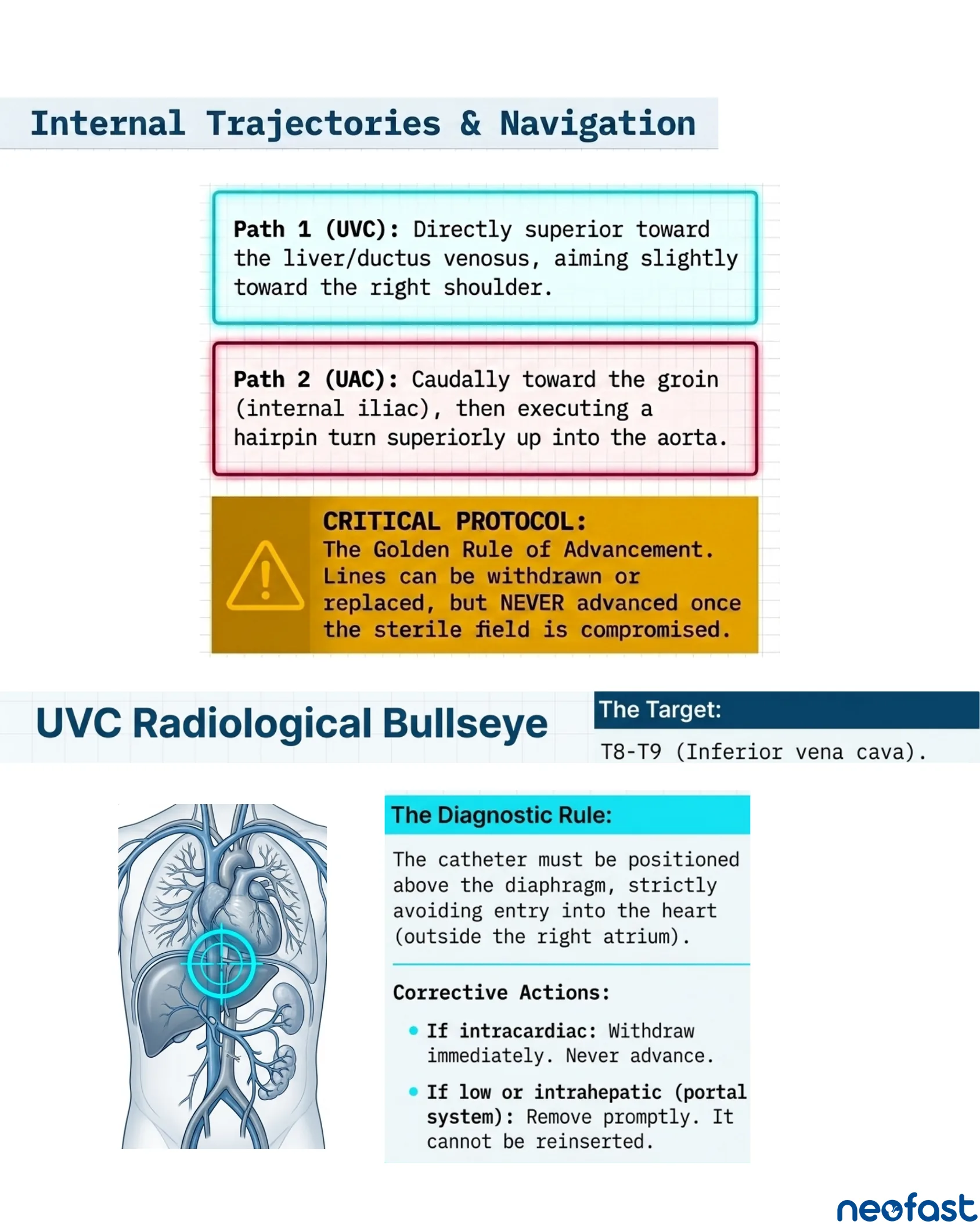
Internal Trajectories & Navigation
Internal Trajectories & Navigation
- Path 1 (UVC): Directly superior toward the liver/ductus venosus, aiming slightly toward the right shoulder.
- Path 2 (UAC): Caudally toward the groin (internal iliac), then executing a hairpin turn superiorly up into the aorta.
CRITICAL PROTOCOL: The Golden Rule of Advancement. Lines can be withdrawn or replaced, but NEVER advanced once the sterile field is compromised.
UVC Radiological Bullseye
The Target: T8-T9 (Inferior vena cava).
The Diagnostic Rule: The catheter must be positioned above the diaphragm, strictly avoiding entry into the heart (outside the right atrium).
Corrective Actions:
- If intracardiac: Withdraw immediately. Never advance.
- If low or intrahepatic (portal system): Remove promptly. It cannot be reinserted.
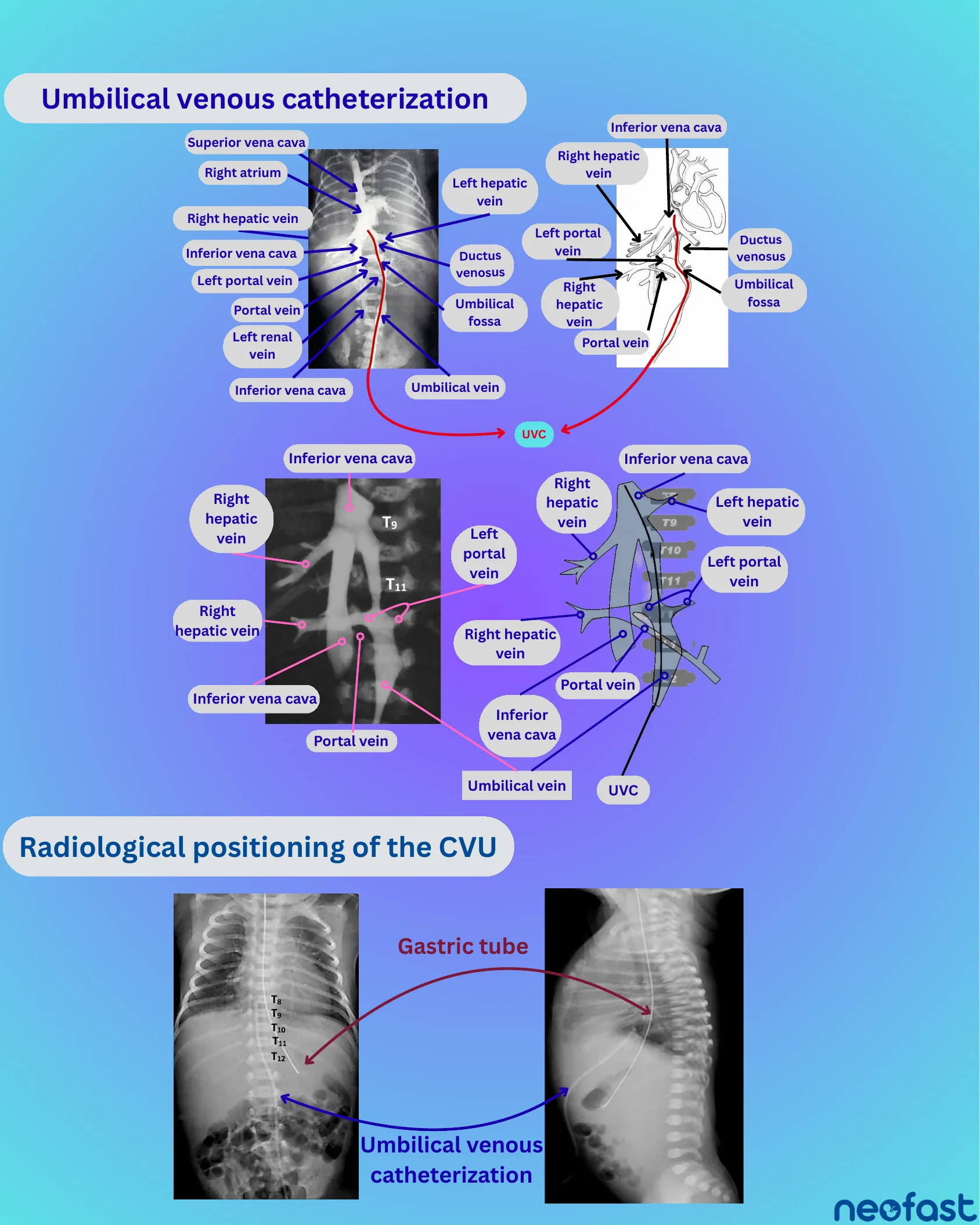
Umbilical Venous Catheterization
Umbilical venous catheterization
Labeled anatomical structures: Superior vena cava, Right atrium, Right hepatic vein, Inferior vena cava, Left portal vein, Portal vein, Left renal vein, Umbilical fossa, Ductus venosus, Umbilical vein → UVC.
Radiograph and diagram show vertebral levels T9 and T11 in relation to the inferior vena cava, hepatic veins, and portal vein pathway of the UVC.
Radiological positioning of the CVU
Vertebral level markers shown: T8, T9, T10, T11, T12.
Frontal and lateral radiographs show correct positioning of the Umbilical venous catheterization line and a Gastric tube.
UAC Radiological Bullseye

UAC Radiological Bullseye
High position: T6 and T9
Low position: L4 and L5
The Target
- High Target Position: T6 to T9.
- Low Target Position: L3 to L4 (or L4-L5).
The Diagnostic Rule
Extends to the iliac artery before entering the aorta. Must be positioned outside the renal artery and other significant arterial branches (above the aortic bifurcation).
Corrective Actions
Remove immediately if mispositioned, or if clinical signs of cyanosis or pallor are noted in the lower limbs. (Maintained for up to 5 days max in absence of complications).
Radiographs show vertebral levels T6, T9, T12, with UVC and UAC catheters labeled, along with landmarks including Left portal vein, Right hepatic vein, Portal vein, and Gastric tube.
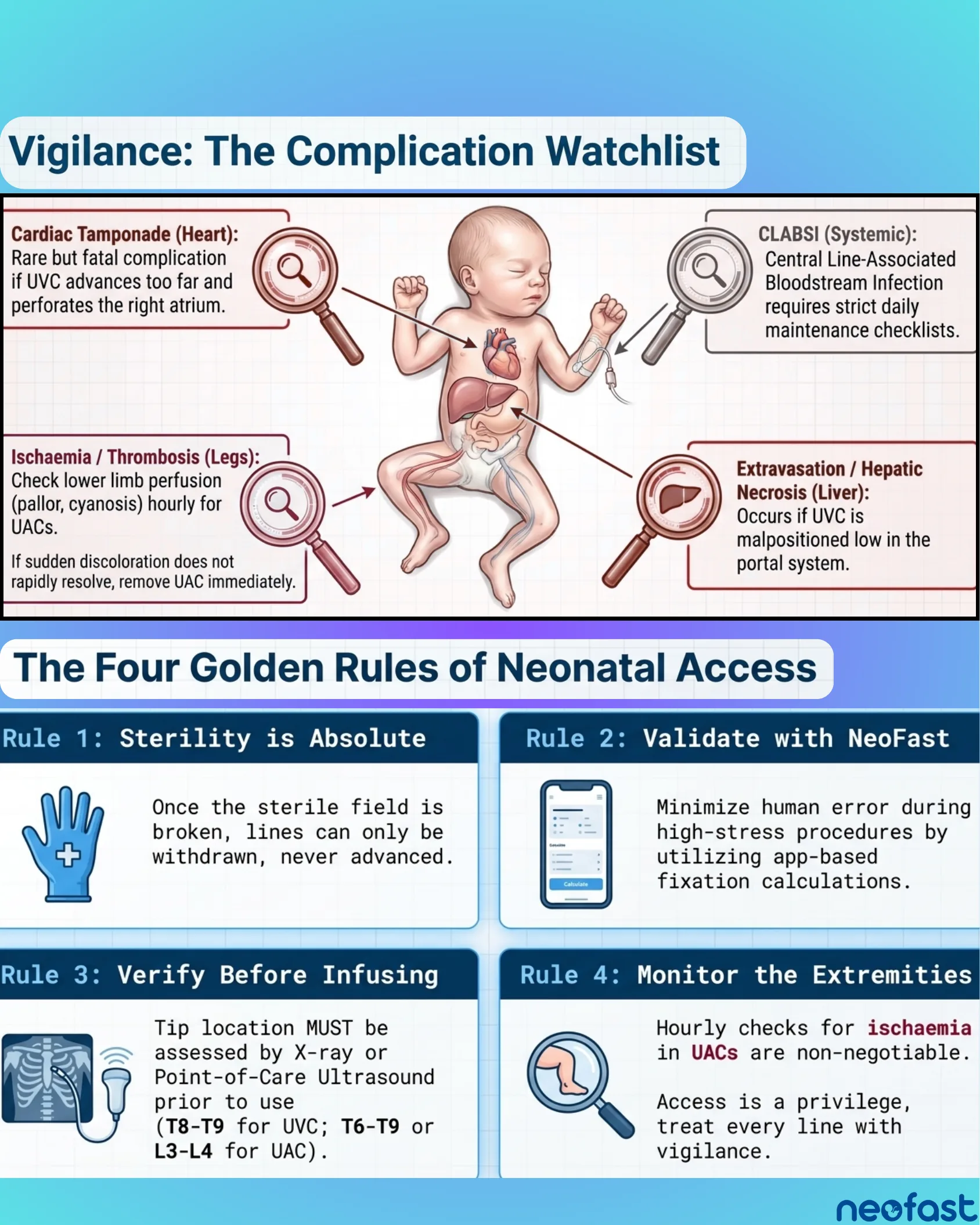
Vigilance: The Complication Watchlist
Vigilance: The Complication Watchlist
Cardiac Tamponade (Heart): Rare but fatal complication if UVC advances too far and perforates the right atrium.
CLABSI (Systemic): Central Line-Associated Bloodstream Infection requires strict daily maintenance checklists.
Ischaemia / Thrombosis (Legs): Check lower limb perfusion (pallor, cyanosis) hourly for UACs.
If sudden discoloration does not rapidly resolve, remove UAC immediately.
Extravasation / Hepatic Necrosis (Liver): Occurs if UVC is malpositioned low in the portal system.
The Four Golden Rules of Neonatal Access
- Rule 1: Sterility is Absolute — Once the sterile field is broken, lines can only be withdrawn, never advanced.
- Rule 2: Validate with NeoFast — Minimize human error during high-stress procedures by utilizing app-based fixation calculations.
- Rule 3: Verify Before Infusing — Tip location MUST be assessed by X-ray or Point-of-Care Ultrasound prior to use (T8-T9 for UVC; T6-T9 or L3-L4 for UAC).
- Rule 4: Monitor the Extremities — Hourly checks for ischaemia in UACs are non-negotiable. Access is a privilege, treat every line with vigilance.
NeoFast App
NeoFast
Neonatal prescribing and much more
Available in 178 countries
- Download on the App Store
- Get it on Google Play