
Cover
Cognitive Aid & Pharmacology Reference
Pediatric & Neonatal Rapid Sequence Intubation
High-Yield Clinical Quick-Reference based on The Harriet Lane Handbook, 24th Edition.
The Four Phases of RSI
The Four Phases of RSI
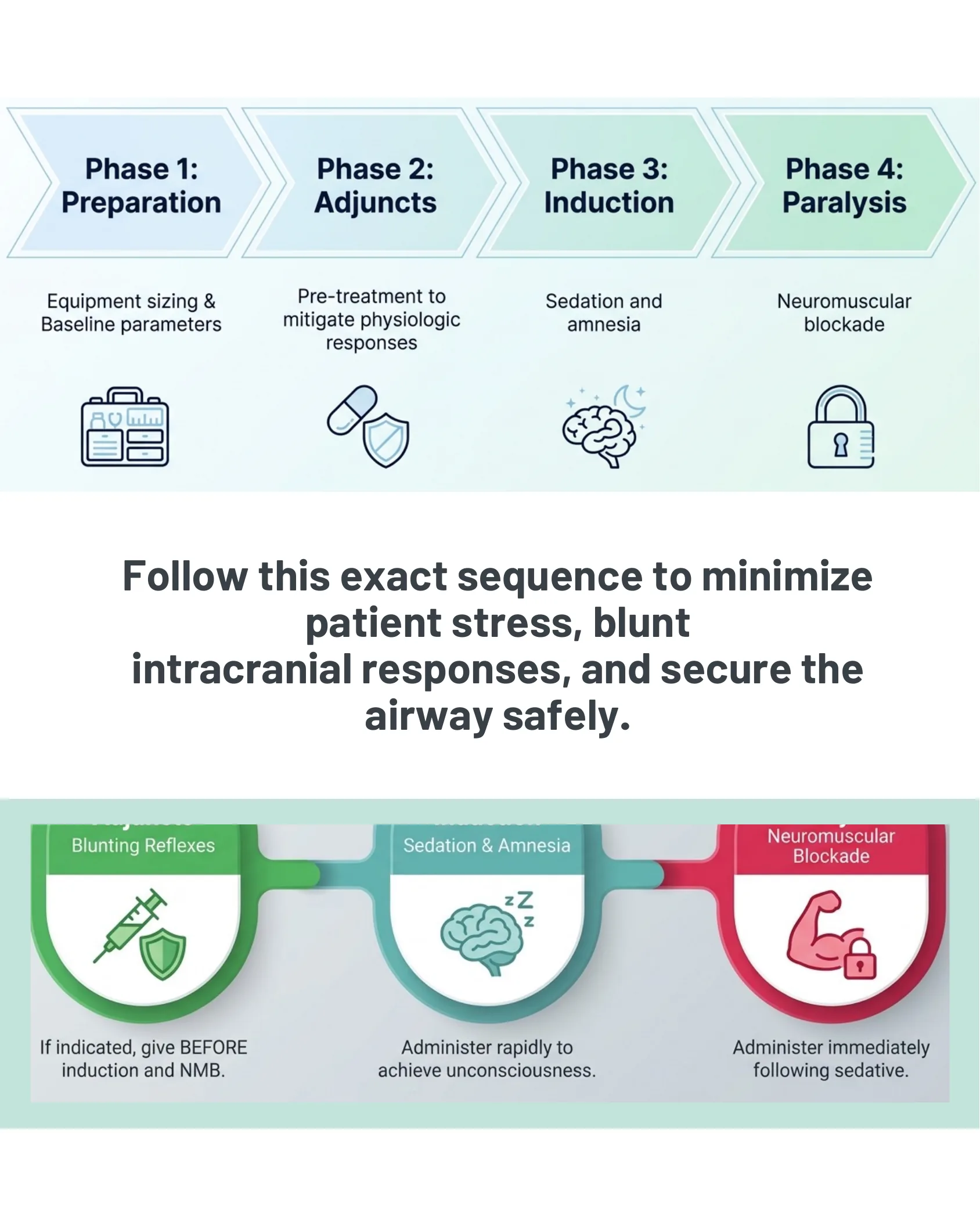
- Phase 1: Preparation — Equipment sizing & baseline parameters.
- Phase 2: Adjuncts — Pre-treatment to mitigate physiologic responses.
- Phase 3: Induction — Sedation and amnesia.
- Phase 4: Paralysis — Neuromuscular blockade.
Follow this exact sequence to minimize patient stress, blunt intracranial responses, and secure the airway safely.
- Adjuncts (Blunting Reflexes): If indicated, give BEFORE induction and NMB.
- Induction (Sedation & Amnesia): Administer rapidly to achieve unconsciousness.
- Paralysis (Neuromuscular Blockade): Administer immediately following sedative.
Equipment Sizing by Age/Weight
Equipment Sizing
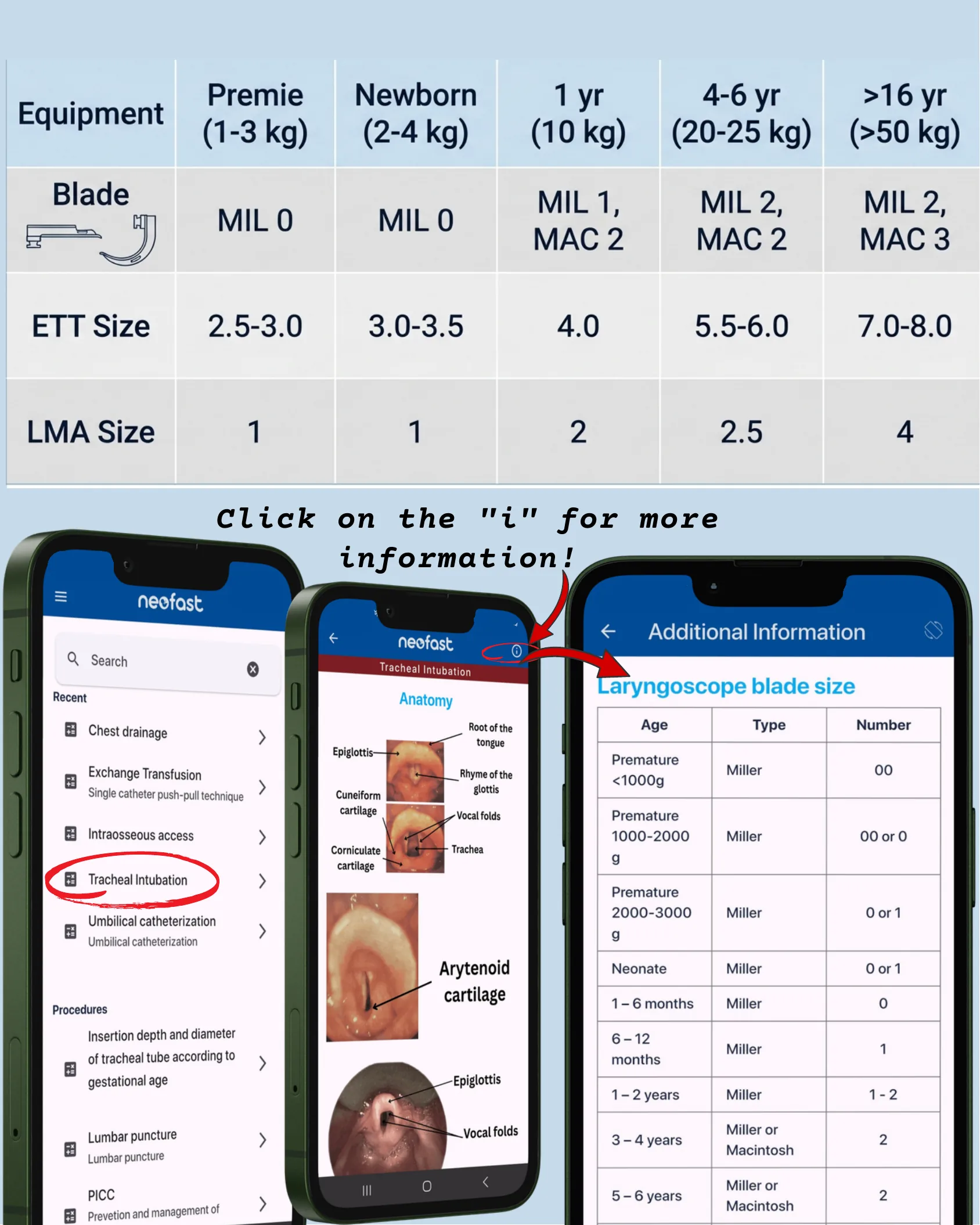
| Equipment | Premie (1-3 kg) | Newborn (2-4 kg) | 1 yr (10 kg) | 4-6 yr (20-25 kg) | >16 yr (>50 kg) |
|---|---|---|---|---|---|
| Blade | MIL 0 | MIL 0 | MIL 1, MAC 2 | MIL 2, MAC 2 | MIL 2, MAC 3 |
| ETT Size | 2.5-3.0 | 3.0-3.5 | 4.0 | 5.5-6.0 | 7.0-8.0 |
| LMA Size | 1 | 1 | 2 | 2.5 | 4 |
Click on the “i” for more information!
Laryngoscope blade size (Additional Information)
| Age | Type | Number |
|---|---|---|
| Premature <1000g | Miller | 00 |
| Premature 1000-2000 g | Miller | 00 or 0 |
| Premature 2000-3000 g | Miller | 0 or 1 |
| Neonate | Miller | 0 or 1 |
| 1 – 6 months | Miller | 0 |
| 6 – 12 months | Miller | 1 |
| 1 – 2 years | Miller | 1 – 2 |
| 3 – 4 years | Miller or Macintosh | 2 |
| 5 – 6 years | Miller or Macintosh | 2 |
Phase 1: RSI Adjuncts (Pre-Medication) — Atropine
Phase 1: RSI Adjuncts (Pre-Medication) — Atropine
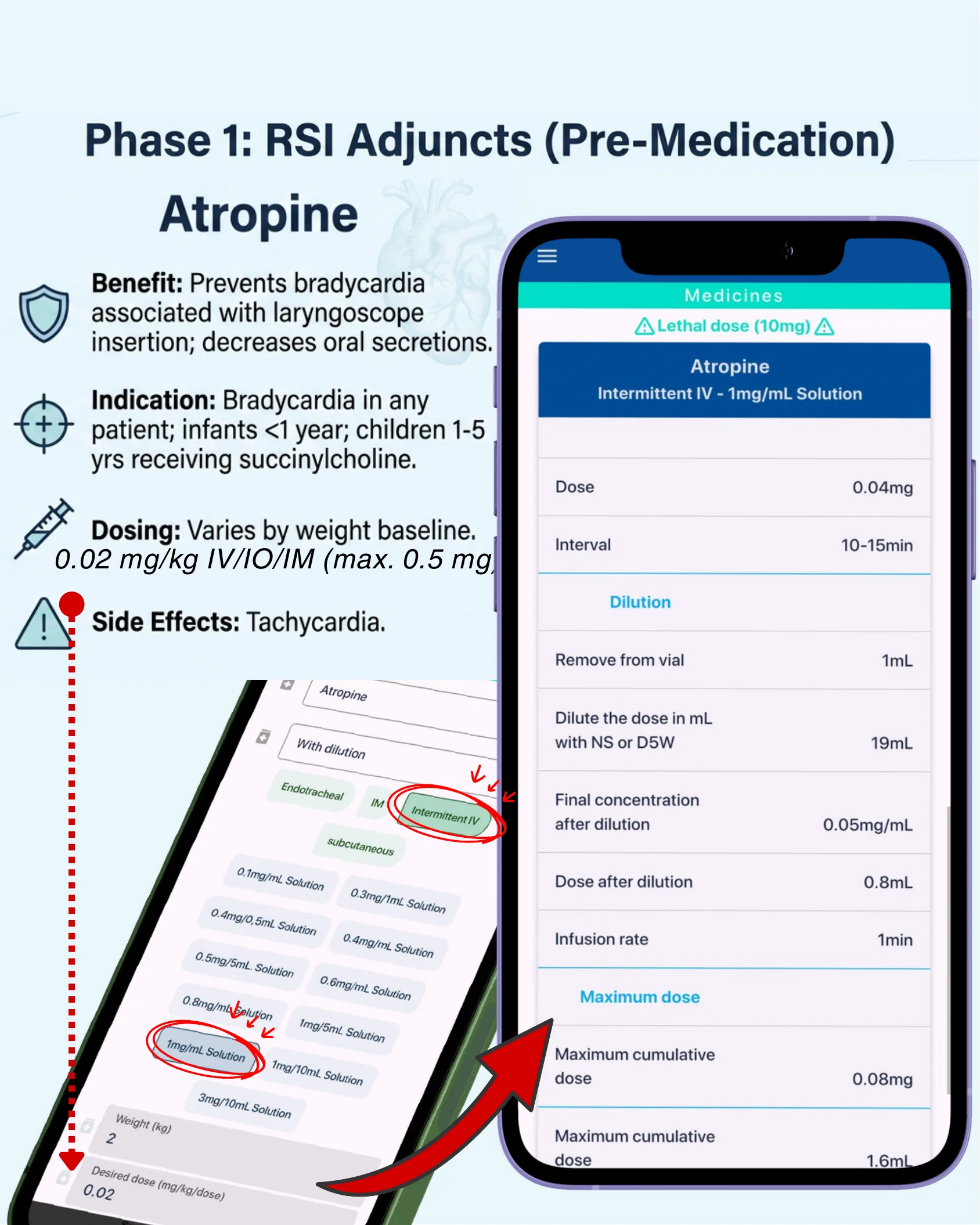
- Benefit: Prevents bradycardia associated with laryngoscope insertion; decreases oral secretions.
- Indication: Bradycardia in any patient; infants <1 year; children 1-5 yrs receiving succinylcholine.
- Dosing: Varies by weight baseline. 0.02 mg/kg IV/IO/IM (max. 0.5 mg).
- Side Effects: Tachycardia.
App: Atropine — Intermittent IV – 1mg/mL Solution
⚠ Lethal dose (10mg) ⚠
| Dose | 0.04mg |
| Interval | 10-15min |
Dilution
| Remove from vial | 1mL |
| Dilute the dose in mL with NS or D5W | 19mL |
| Final concentration after dilution | 0.05mg/mL |
| Dose after dilution | 0.8mL |
| Infusion rate | 1min |
Maximum dose
| Maximum cumulative dose | 0.08mg |
| Maximum cumulative dose | 1.6mL |
Phase 1: RSI Adjuncts (Pre-Medication) — Lidocaine
Phase 1: RSI Adjuncts (Pre-Medication) — Lidocaine
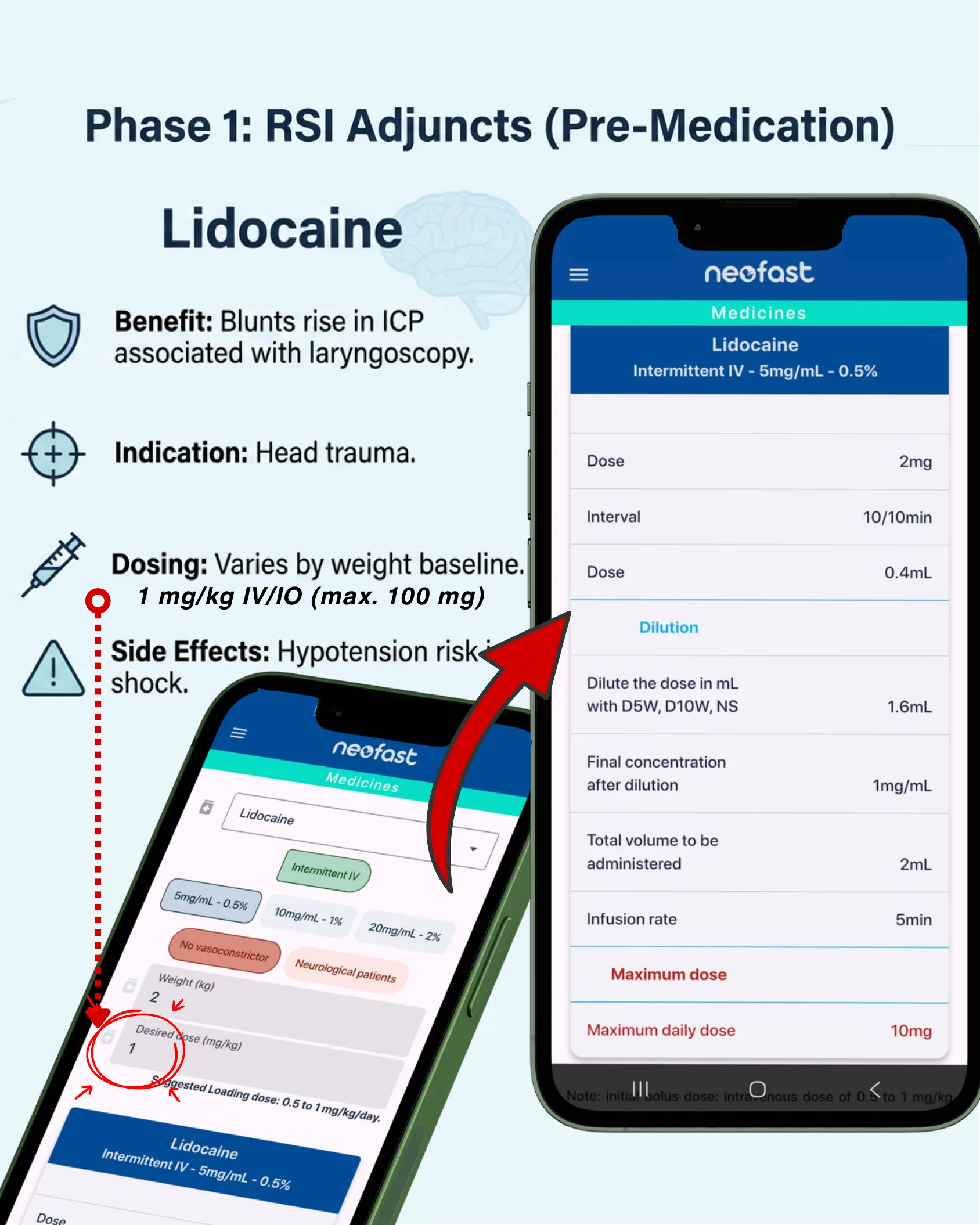
- Benefit: Blunts rise in ICP associated with laryngoscopy.
- Indication: Head trauma.
- Dosing: Varies by weight baseline. 1 mg/kg IV/IO (max. 100 mg).
- Side Effects: Hypotension risk in shock.
App: Lidocaine — Intermittent IV – 5mg/mL – 0.5%
| Dose | 2mg |
| Interval | 10/10min |
| Dose | 0.4mL |
Dilution
| Dilute the dose in mL with D5W, D10W, NS | 1.6mL |
| Final concentration after dilution | 1mg/mL |
| Total volume to be administered | 2mL |
| Infusion rate | 5min |
Maximum dose
| Maximum daily dose | 10mg |
App input options: Intermittent IV; 5mg/mL – 0.5%, 10mg/mL – 1%, 20mg/mL – 2%; No vasoconstrictor; Neurological patients. Suggested Loading dose: 0.5 to 1 mg/kg/day.
Note: initial bolus dose: intravenous dose of 0.5 to 1 mg/kg.
Phase 2: Induction Agents (Hemodynamic Profiles) — Fentanyl
Phase 2: Induction Agents (Hemodynamic Profiles) — Fentanyl
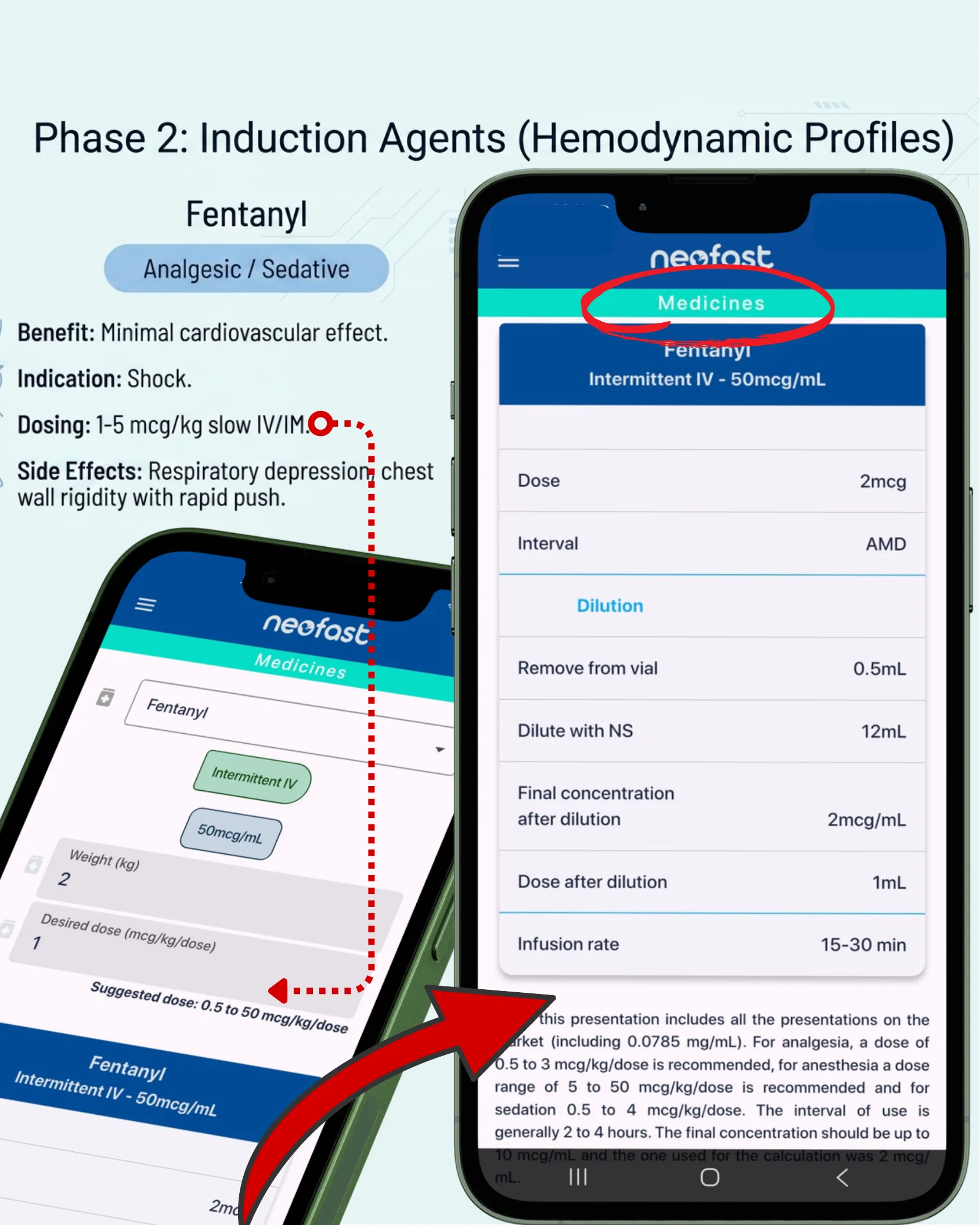
Analgesic / Sedative
- Benefit: Minimal cardiovascular effect.
- Indication: Shock.
- Dosing: 1-5 mcg/kg slow IV/IM.
- Side Effects: Respiratory depression, chest wall rigidity with rapid push.
App: Fentanyl — Intermittent IV – 50mcg/mL
| Dose | 2mcg |
| Interval | AMD |
Dilution
| Remove from vial | 0.5mL |
| Dilute with NS | 12mL |
| Final concentration after dilution | 2mcg/mL |
| Dose after dilution | 1mL |
| Infusion rate | 15-30 min |
App input: Weight (kg) 2; Desired dose (mcg/kg/dose) 1. Suggested dose: 0.5 to 50 mcg/kg/dose.
Note: this presentation includes all the presentations on the market (including 0.0785 mg/mL). For analgesia, a dose of 0.5 to 3 mcg/kg/dose is recommended, for anesthesia a dose range of 5 to 50 mcg/kg/dose is recommended and for sedation 0.5 to 4 mcg/kg/dose. The interval of use is generally 2 to 4 hours. The final concentration should be up to 10 mcg/mL and the one used for the calculation was 2 mcg/mL.
How to Use the App for Intubation Medications
Two ways to select intubation medications
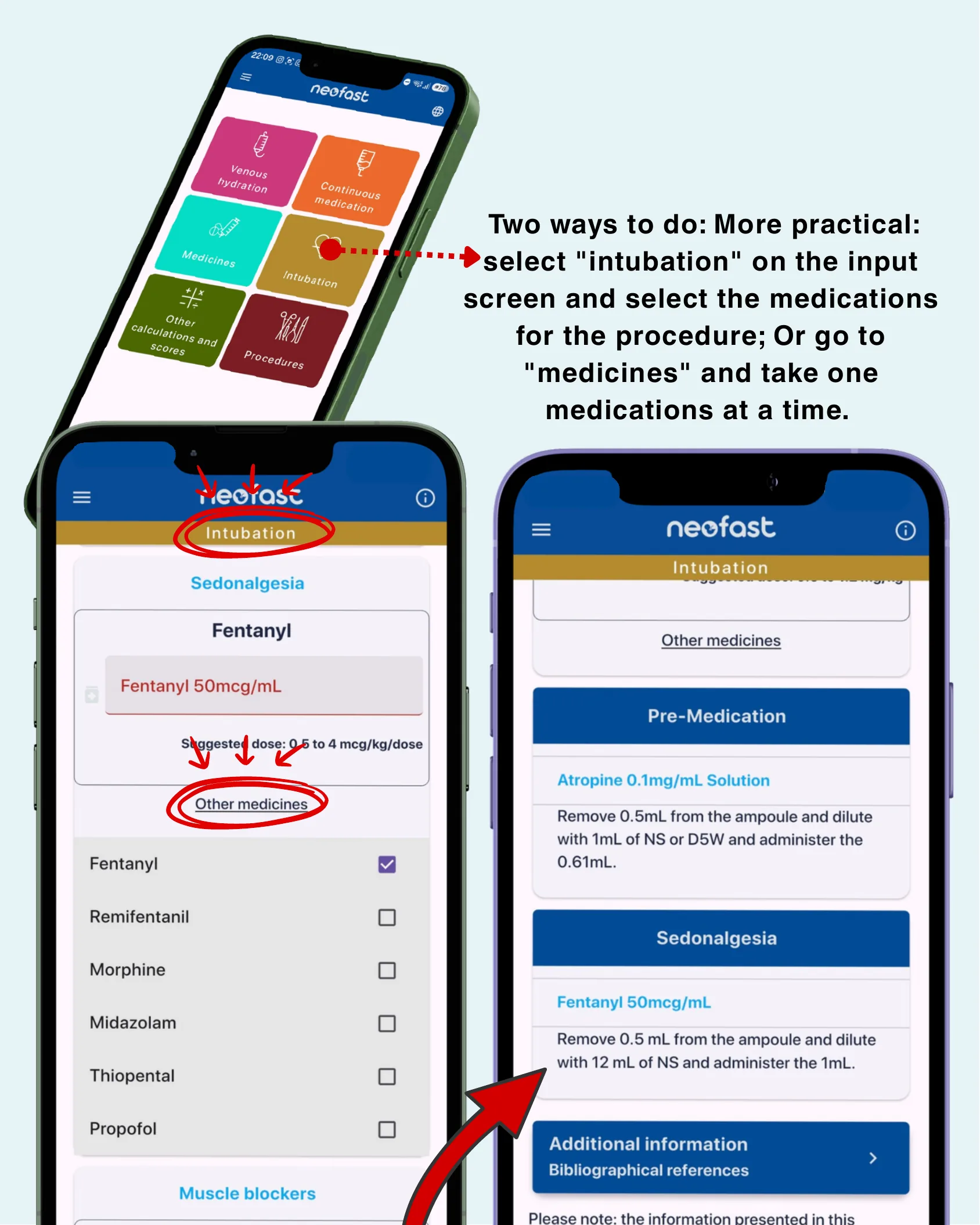
Two ways to do: More practical: select “intubation” on the input screen and select the medications for the procedure; Or go to “medicines” and take one medications at a time.
Home menu options: Venous hydration; Continuous medication; Medicines; Intubation; Other calculations and scores; Procedures.
Intubation — Sedonalgesia
Fentanyl — Fentanyl 50mcg/mL. Suggested dose: 0.5 to 4 mcg/kg/dose.
Other medicines: Fentanyl (selected), Remifentanil, Morphine, Midazolam, Thiopental, Propofol, Muscle blockers.
Results screen
Pre-Medication — Atropine 0.1mg/mL Solution: Remove 0.5mL from the ampoule and dilute with 1mL of NS or D5W and administer the 0.61mL.
Sedonalgesia — Fentanyl 50mcg/mL: Remove 0.5 mL from the ampoule and dilute with 12 mL of NS and administer the 1mL.
Additional information: Bibliographical references.
Please note: the information presented in this…
Phase 2: Induction Agents (Short-Acting Profile) — Midazolam
Phase 2: Induction Agents (Short-Acting Profile) — Midazolam
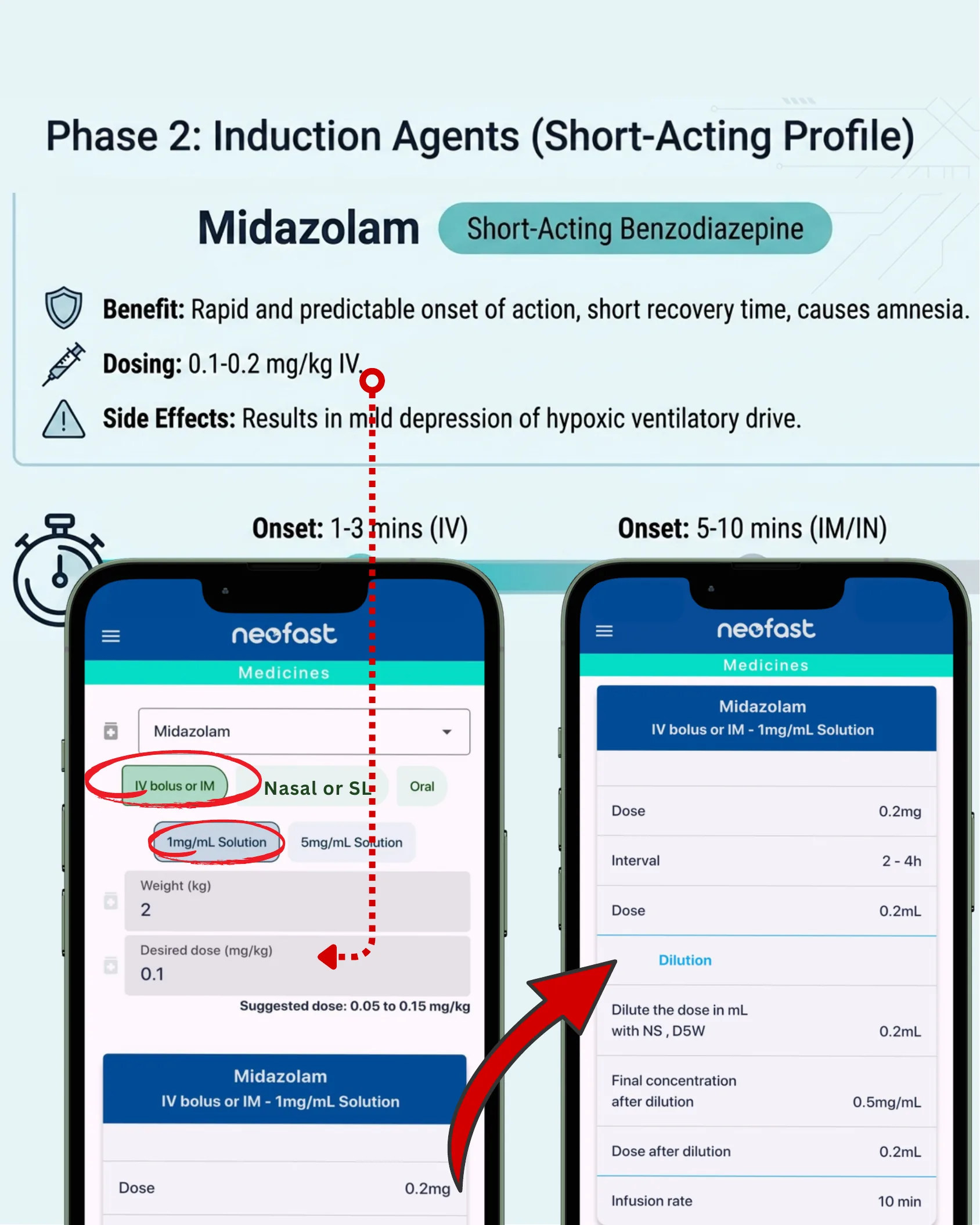
Short-Acting Benzodiazepine
- Benefit: Rapid and predictable onset of action, short recovery time, causes amnesia.
- Dosing: 0.1-0.2 mg/kg IV.
- Side Effects: Results in mild depression of hypoxic ventilatory drive.
- Onset: 1-3 mins (IV)
- Onset: 5-10 mins (IM/IN)
App input options: IV bolus or IM; Nasal or SL; Oral. Solutions: 1mg/mL Solution, 5mg/mL Solution. Weight (kg) 2; Desired dose (mg/kg) 0.1. Suggested dose: 0.05 to 0.15 mg/kg.
App: Midazolam — IV bolus or IM – 1mg/mL Solution
| Dose | 0.2mg |
| Interval | 2 – 4h |
| Dose | 0.2mL |
Dilution
| Dilute the dose in mL with NS, D5W | 0.2mL |
| Final concentration after dilution | 0.5mg/mL |
| Dose after dilution | 0.2mL |
| Infusion rate | 10 min |
Phase 3: Neuromuscular Blockade (Depolarizing)
Phase 3: Neuromuscular Blockade (Depolarizing)
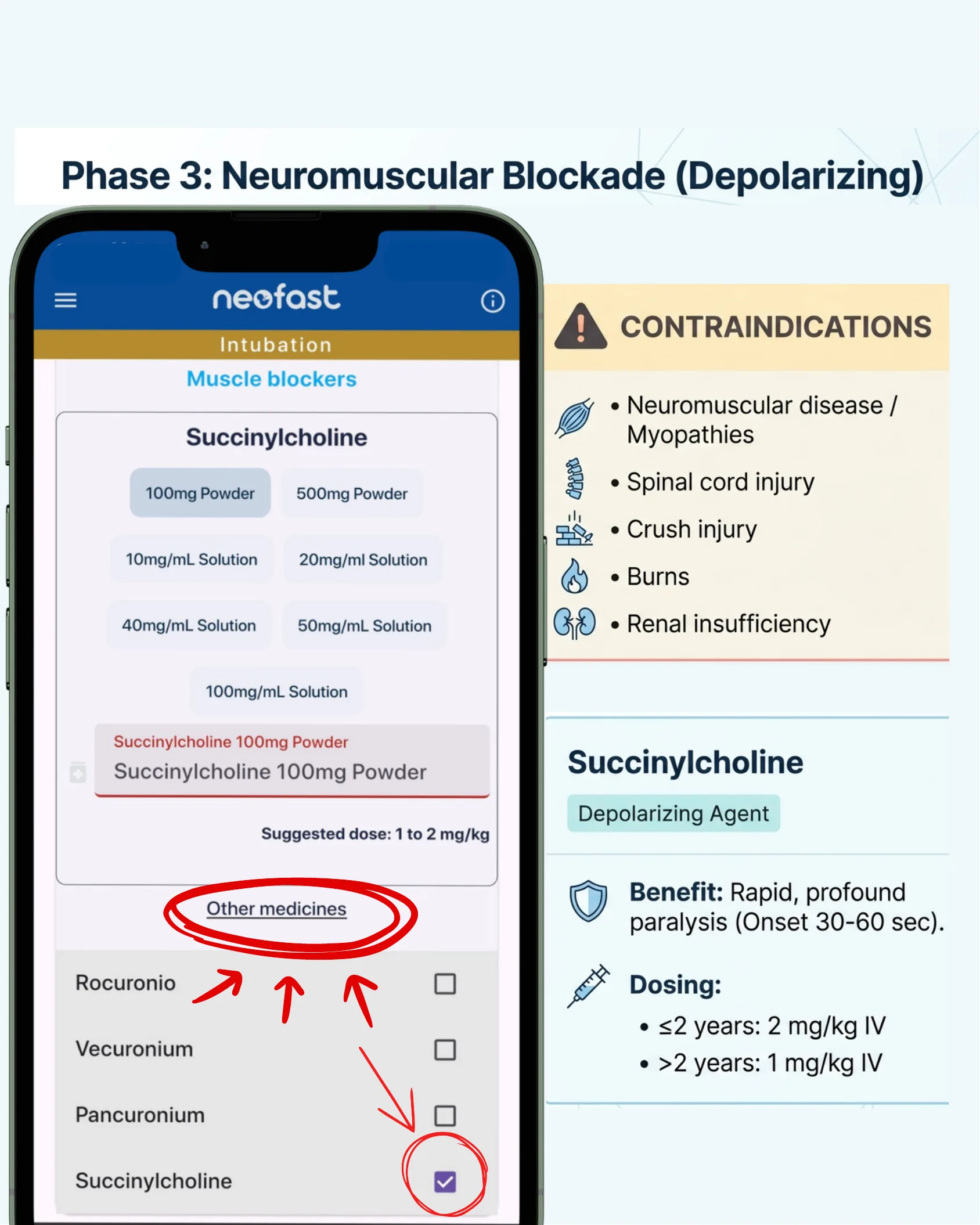
App view — Intubation / Muscle blockers
Succinylcholine
Available formulations:
- 100mg Powder
- 500mg Powder
- 10mg/mL Solution
- 20mg/ml Solution
- 40mg/mL Solution
- 50mg/mL Solution
- 100mg/mL Solution
Selected: Succinylcholine 100mg Powder
Suggested dose: 1 to 2 mg/kg
Other medicines: Rocuronio, Vecuronium, Pancuronium, Succinylcholine (selected)
Contraindications
- Neuromuscular disease / Myopathies
- Spinal cord injury
- Crush injury
- Burns
- Renal insufficiency
Succinylcholine — Depolarizing Agent
Benefit: Rapid, profound paralysis (Onset 30-60 sec).
Dosing:
- ≤2 years: 2 mg/kg IV
- >2 years: 1 mg/kg IV
Rocuronium Bromide Injection
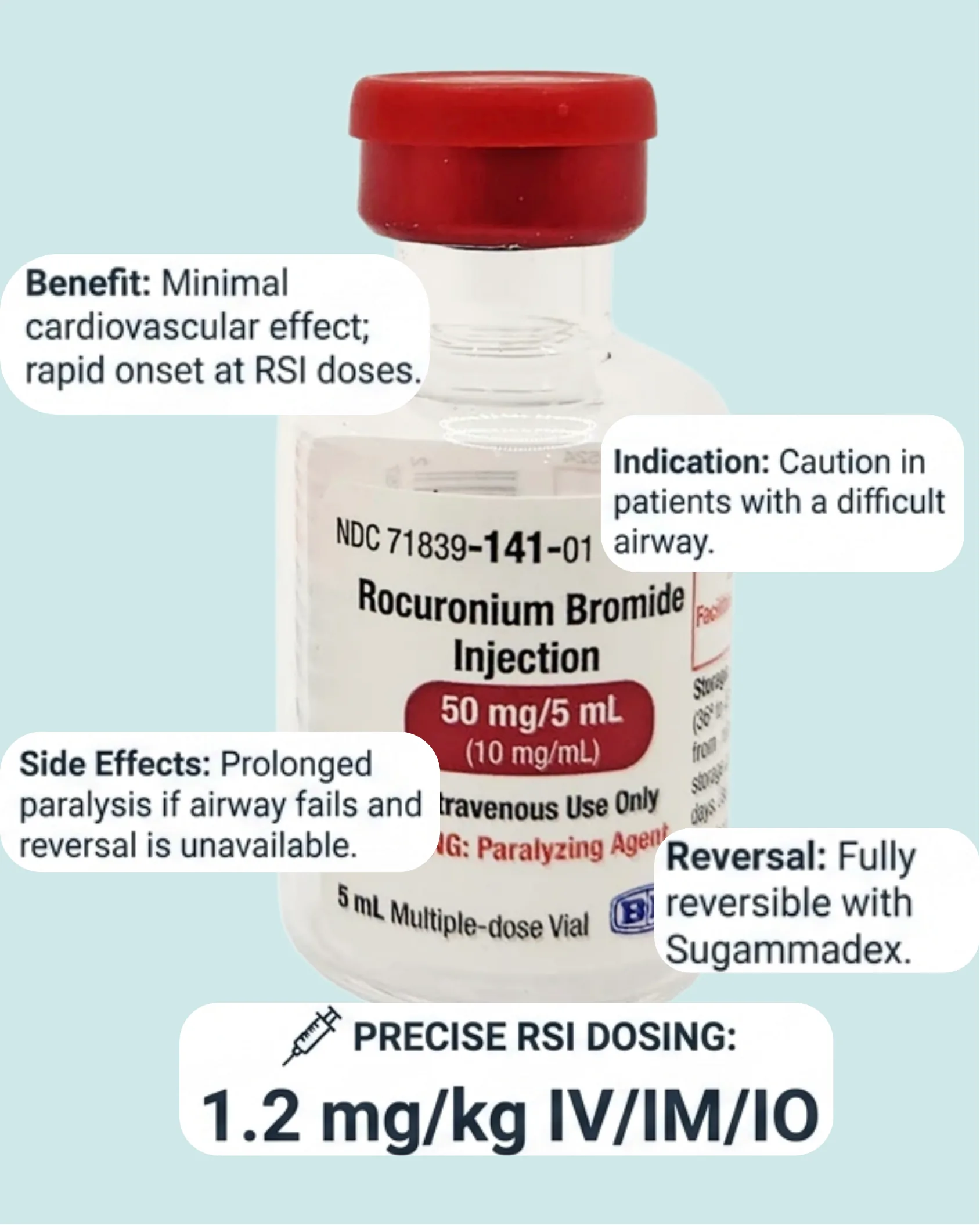
Rocuronium Bromide Injection
NDC 71839-141-01
Rocuronium Bromide Injection — 50 mg/5 mL (10 mg/mL). Intravenous Use Only. WARNING: Paralyzing Agent. 5 mL Multiple-dose Vial.
Benefit: Minimal cardiovascular effect; rapid onset at RSI doses.
Indication: Caution in patients with a difficult airway.
Side Effects: Prolonged paralysis if airway fails and reversal is unavailable.
Reversal: Fully reversible with Sugammadex.
Precise RSI Dosing: 1.2 mg/kg IV/IM/IO
Rocuronio and Vecuronium App View
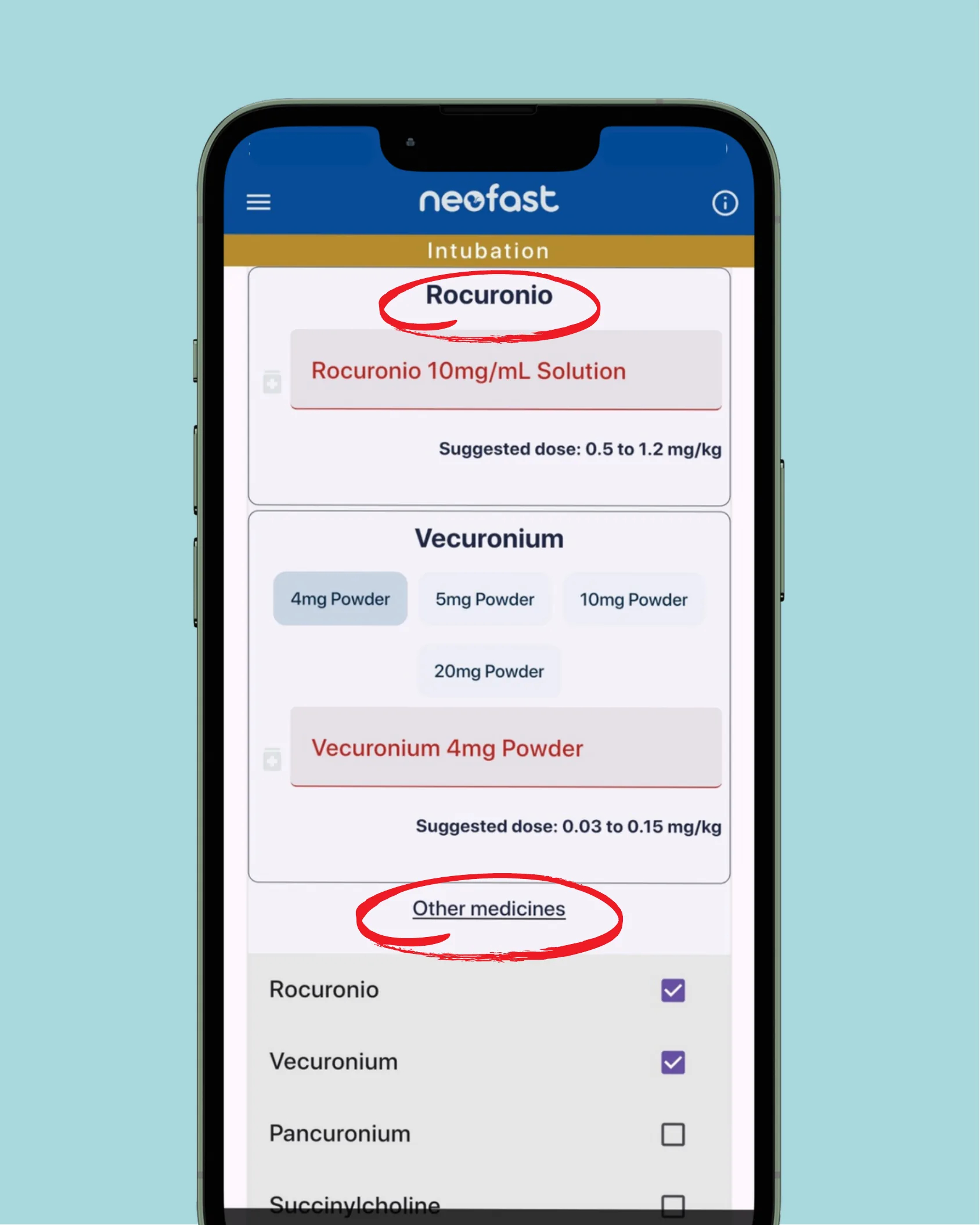
Neofast — Intubation
Rocuronio
Selected: Rocuronio 10mg/mL Solution
Suggested dose: 0.5 to 1.2 mg/kg
Vecuronium
Available formulations:
- 4mg Powder
- 5mg Powder
- 10mg Powder
- 20mg Powder
Selected: Vecuronium 4mg Powder
Suggested dose: 0.03 to 0.15 mg/kg
Other medicines:
- Rocuronio (selected)
- Vecuronium (selected)
- Pancuronium
- Succinylcholine
Phase 3: Neuromuscular Blockade (Non-Depolarizing Alternative)
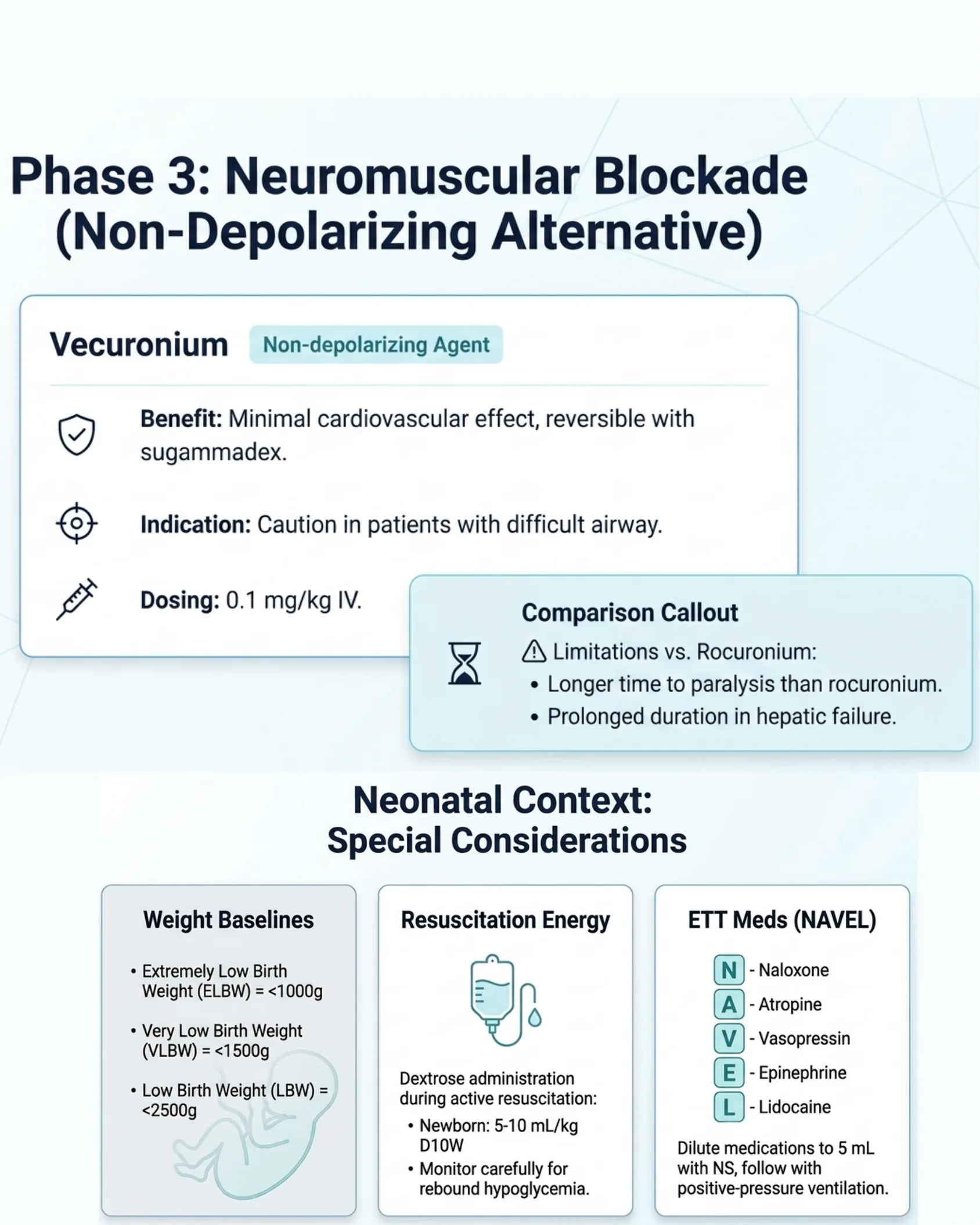
Phase 3: Neuromuscular Blockade (Non-Depolarizing Alternative)
Vecuronium — Non-depolarizing Agent
Benefit: Minimal cardiovascular effect, reversible with sugammadex.
Indication: Caution in patients with difficult airway.
Dosing: 0.1 mg/kg IV.
Comparison Callout
Limitations vs. Rocuronium:
- Longer time to paralysis than rocuronium.
- Prolonged duration in hepatic failure.
Neonatal Context: Special Considerations
Weight Baselines
- Extremely Low Birth Weight (ELBW) = <1000g
- Very Low Birth Weight (VLBW) = <1500g
- Low Birth Weight (LBW) = <2500g
Resuscitation Energy — Dextrose administration during active resuscitation:
- Newborn: 5-10 mL/kg D10W
- Monitor carefully for rebound hypoglycemia.
ETT Meds (NAVEL)
- N – Naloxone
- A – Atropine
- V – Vasopressin
- E – Epinephrine
- L – Lidocaine
Dilute medications to 5 mL with NS, follow with positive-pressure ventilation.
Master Synthesis: RSI Pharmacologic Cheat Sheet
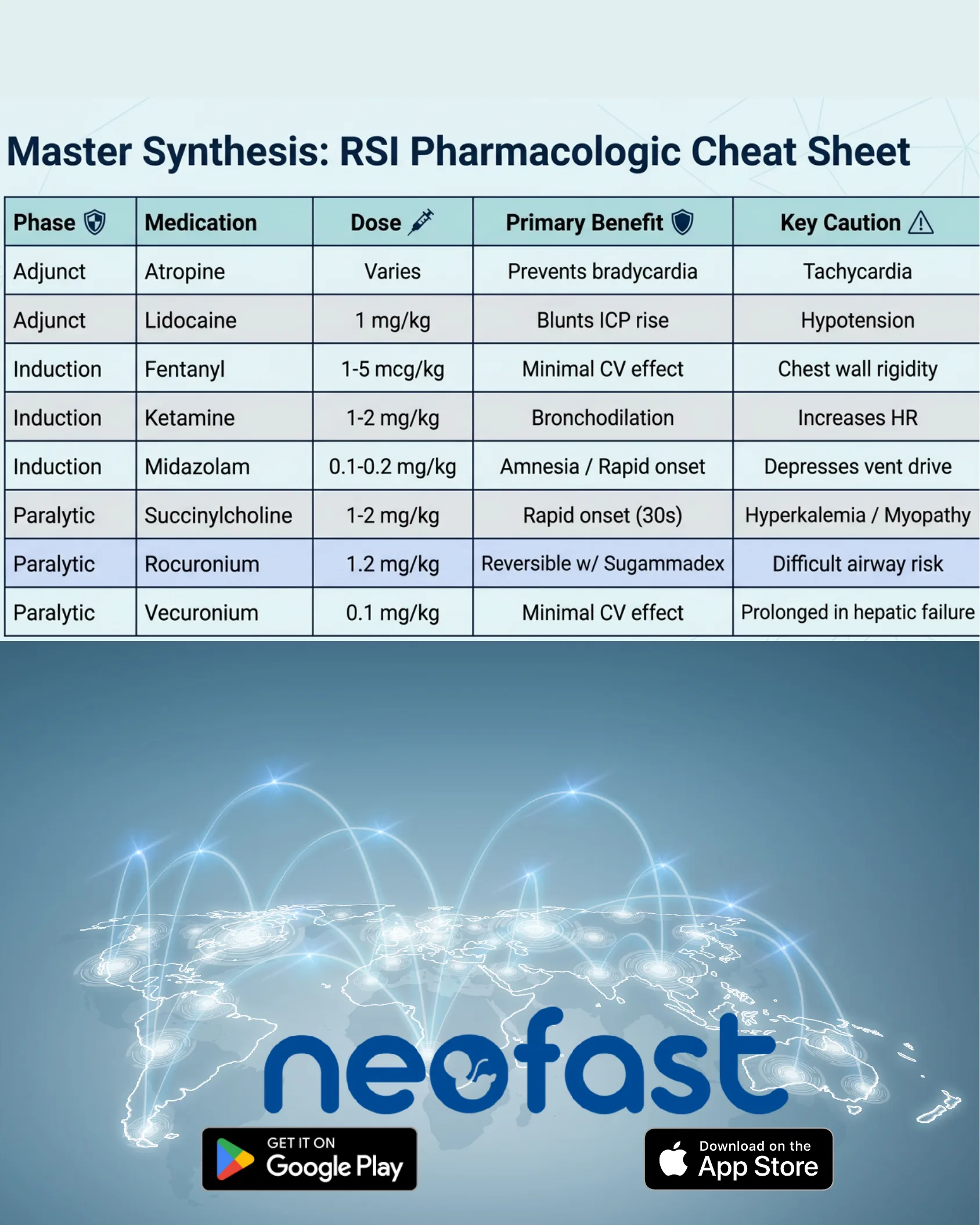
Master Synthesis: RSI Pharmacologic Cheat Sheet
| Phase | Medication | Dose | Primary Benefit | Key Caution |
|---|---|---|---|---|
| Adjunct | Atropine | Varies | Prevents bradycardia | Tachycardia |
| Adjunct | Lidocaine | 1 mg/kg | Blunts ICP rise | Hypotension |
| Induction | Fentanyl | 1-5 mcg/kg | Minimal CV effect | Chest wall rigidity |
| Induction | Ketamine | 1-2 mg/kg | Bronchodilation | Increases HR |
| Induction | Midazolam | 0.1-0.2 mg/kg | Amnesia / Rapid onset | Depresses vent drive |
| Paralytic | Succinylcholine | 1-2 mg/kg | Rapid onset (30s) | Hyperkalemia / Myopathy |
| Paralytic | Rocuronium | 1.2 mg/kg | Reversible w/ Sugammadex | Difficult airway risk |
| Paralytic | Vecuronium | 0.1 mg/kg | Minimal CV effect | Prolonged in hepatic failure |
neofast — Get it on Google Play / Download on the App Store

Phase 1: Adjuncts
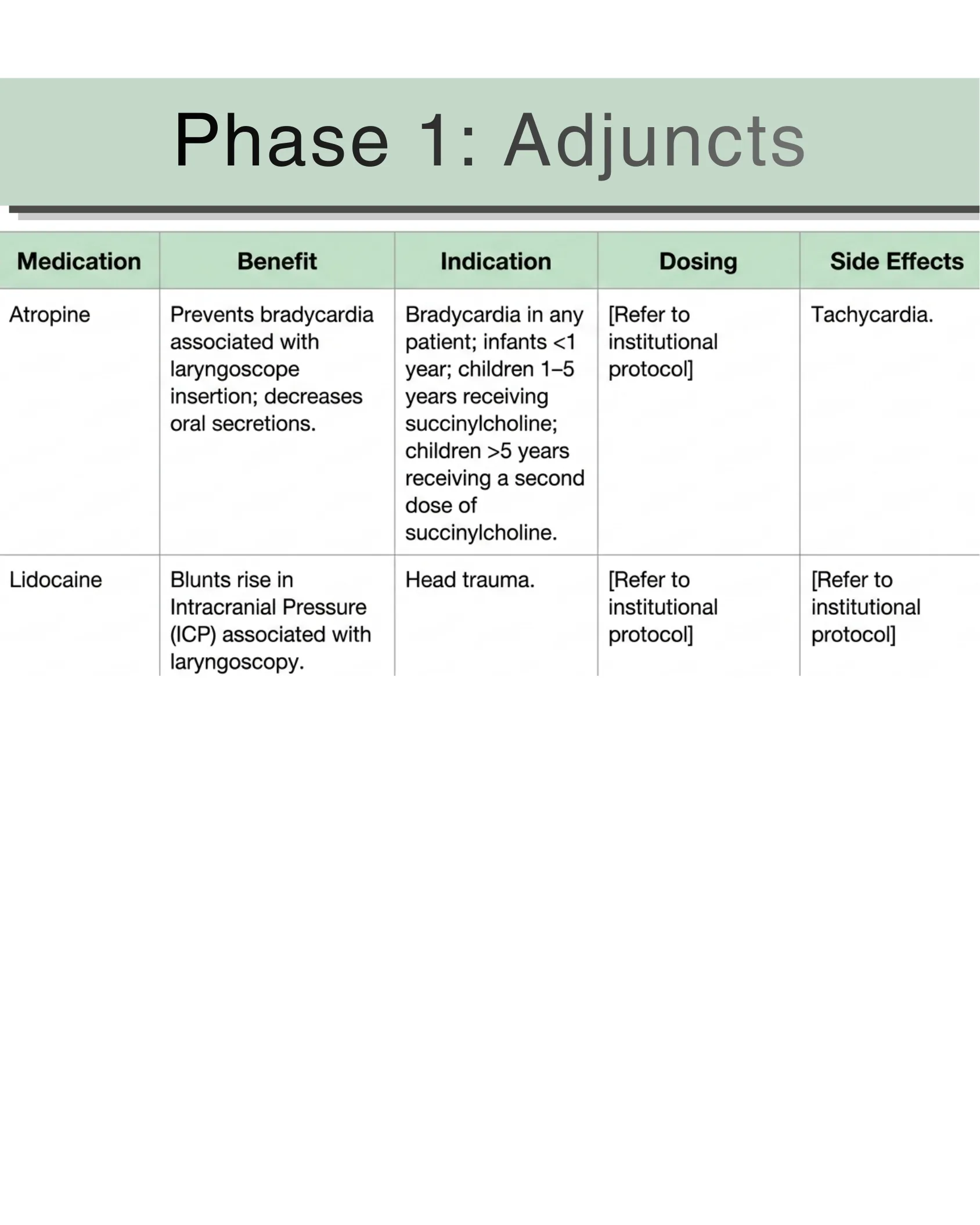
Phase 1: Adjuncts
| Medication | Benefit | Indication | Dosing | Side Effects |
|---|---|---|---|---|
| Atropine | Prevents bradycardia associated with laryngoscope insertion; decreases oral secretions. | Bradycardia in any patient; infants <1 year; children 1–5 years receiving succinylcholine; children >5 years receiving a second dose of succinylcholine. | [Refer to institutional protocol] | Tachycardia. |
| Lidocaine | Blunts rise in Intracranial Pressure (ICP) associated with laryngoscopy. | Head trauma. | [Refer to institutional protocol] | [Refer to institutional protocol] |
Table 1.2 Rapid Sequence Intubation Medications
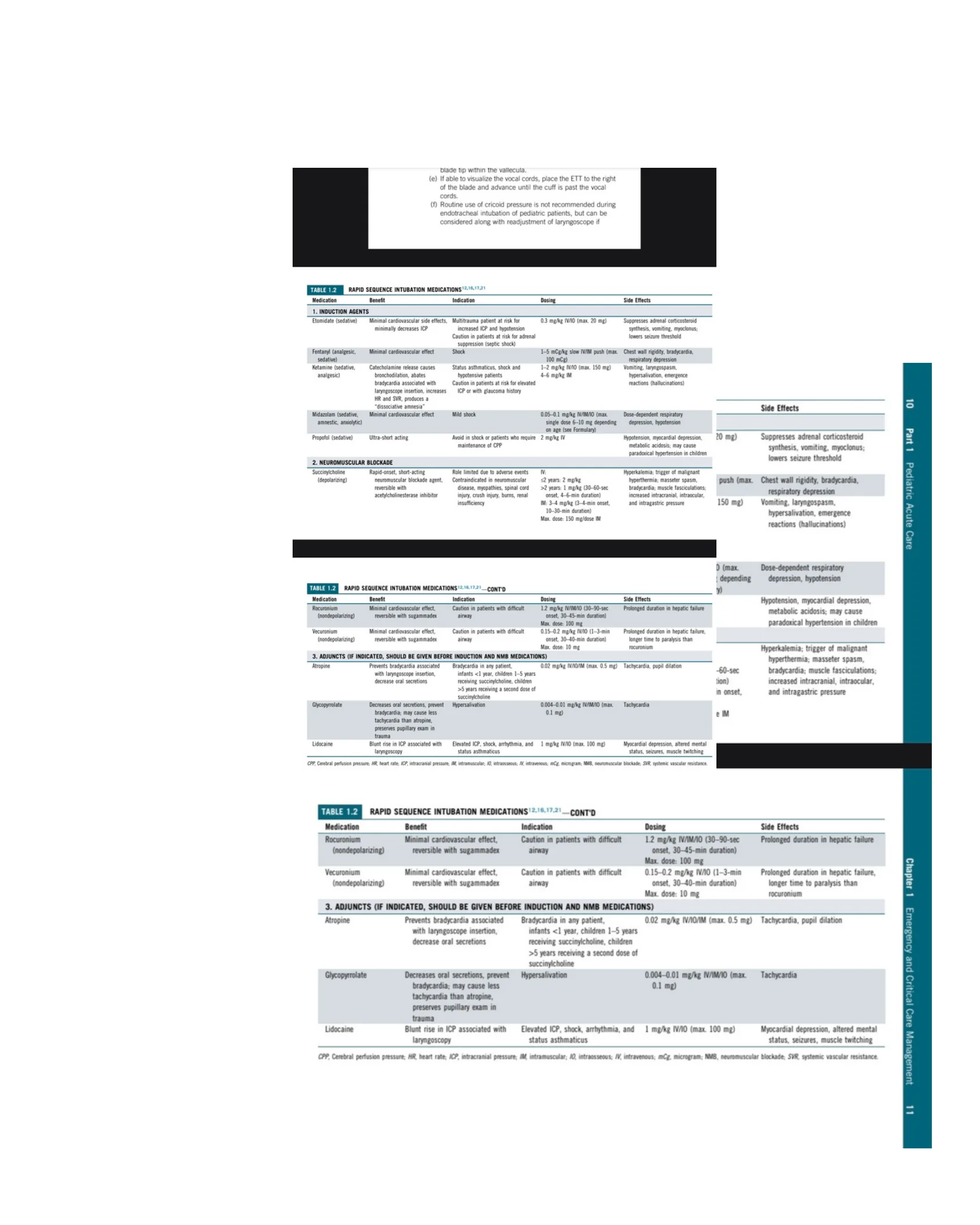
Table 1.2 — Rapid Sequence Intubation Medications
Intubation technique notes: (e) If able to visualize the vocal cords, place the ETT to the right of the blade and advance until the cuff is past the vocal cords. (f) Routine use of cricoid pressure is not recommended during endotracheal intubation of pediatric patients, but can be considered along with readjustment of laryngoscope.
1. Induction Agents
| Medication | Benefit | Indication | Dosing | Side Effects |
|---|---|---|---|---|
| Etomidate (sedative) | Minimal cardiovascular side effects, minimally decreases ICP | Multitrauma patient at risk for increased ICP and hypotension. Caution in patients at risk for adrenal suppression (septic shock) | 0.3 mg/kg IV/IO (max. 20 mg) | Suppresses adrenal corticosteroid synthesis, vomiting, myoclonus; lowers seizure threshold |
| Fentanyl (analgesic, sedative) | Minimal cardiovascular effect | Shock | 1–5 mcg/kg slow IV/IM push (max. 100 mcg) | Chest wall rigidity, bradycardia, respiratory depression |
| Ketamine (sedative, analgesic) | Catecholamine release causes bronchodilation, abates bradycardia associated with laryngoscope insertion, increases HR and SVR, produces a “dissociative amnesia” | Status asthmaticus, shock and hypotensive patients. Caution in patients at risk for elevated ICP or with glaucoma history | 1–2 mg/kg IV/IO (max. 150 mg); 4–6 mg/kg IM | Vomiting, laryngospasm, hypersalivation, emergence reactions (hallucinations) |
| Midazolam (sedative, amnestic, anxiolytic) | Minimal cardiovascular effect | Mild shock | 0.05–0.1 mg/kg IV/IM/IO (max. single dose 6–10 mg depending on age, see Formulary) | Dose-dependent respiratory depression, hypotension |
| Propofol (sedative) | Ultra-short acting | Avoid in shock or patients who require maintenance of CPP | 2 mg/kg IV | Hypotension, myocardial depression, metabolic acidosis; may cause paradoxical hypertension in children |
2. Neuromuscular Blockade
| Medication | Benefit | Indication | Dosing | Side Effects |
|---|---|---|---|---|
| Succinylcholine (depolarizing) | Rapid-onset, short-acting neuromuscular blockade agent, reversible with acetylcholinesterase inhibitor | Role limited due to adverse events. Contraindicated in neuromuscular disease, myopathies, spinal cord injury, crush injury, burns, renal insufficiency | IV: ≤2 years: 2 mg/kg; >2 years: 1 mg/kg (30–60-sec onset, 4–6-min duration). IM: 3–4 mg/kg (3–4-min onset, 10–30-min duration). Max. dose: 150 mg/dose IM | Hyperkalemia; trigger of malignant hyperthermia; masseter spasm, bradycardia; muscle fasciculations; increased intracranial, intraocular, and intragastric pressure |
| Rocuronium (nondepolarizing) | Minimal cardiovascular effect, reversible with sugammadex | Caution in patients with difficult airway | 1.2 mg/kg IV/IM/IO (30–90-sec onset, 30–45-min duration). Max. dose: 100 mg | Prolonged duration in hepatic failure |
| Vecuronium (nondepolarizing) | Minimal cardiovascular effect, reversible with sugammadex | Caution in patients with difficult airway | 0.15–0.2 mg/kg IV/IO (1–3-min onset, 30–40-min duration). Max. dose: 10 mg | Prolonged duration in hepatic failure, longer time to paralysis than rocuronium |
3. Adjuncts (If indicated, should be given before induction and NMB medications)
| Medication | Benefit | Indication | Dosing | Side Effects |
|---|---|---|---|---|
| Atropine | Prevents bradycardia associated with laryngoscope insertion, decrease oral secretions | Bradycardia in any patient, infants <1 year, children 1–5 years receiving succinylcholine, children >5 years receiving a second dose of succinylcholine | 0.02 mg/kg IV/IO/IM (max. 0.5 mg) | Tachycardia, pupil dilation |
| Glycopyrrolate | Decreases oral secretions, prevent bradycardia; may cause less tachycardia than atropine, preserves pupillary exam in trauma | Hypersalivation | 0.004–0.01 mg/kg IV/IM/IO (max. 0.1 mg) | Tachycardia |
| Lidocaine | Blunt rise in ICP associated with laryngoscopy | Elevated ICP, shock, arrhythmia, and status asthmaticus | 1 mg/kg IV/IO (max. 100 mg) | Myocardial depression, altered mental status, seizures, muscle twitching |
CPP, Cerebral perfusion pressure; HR, heart rate; ICP, intracranial pressure; IM, intramuscular; IO, intraosseous; IV, intravenous; mcg, microgram; NMB, neuromuscular blockade; SVR, systemic vascular resistance.
Phase 2: Induction Agents
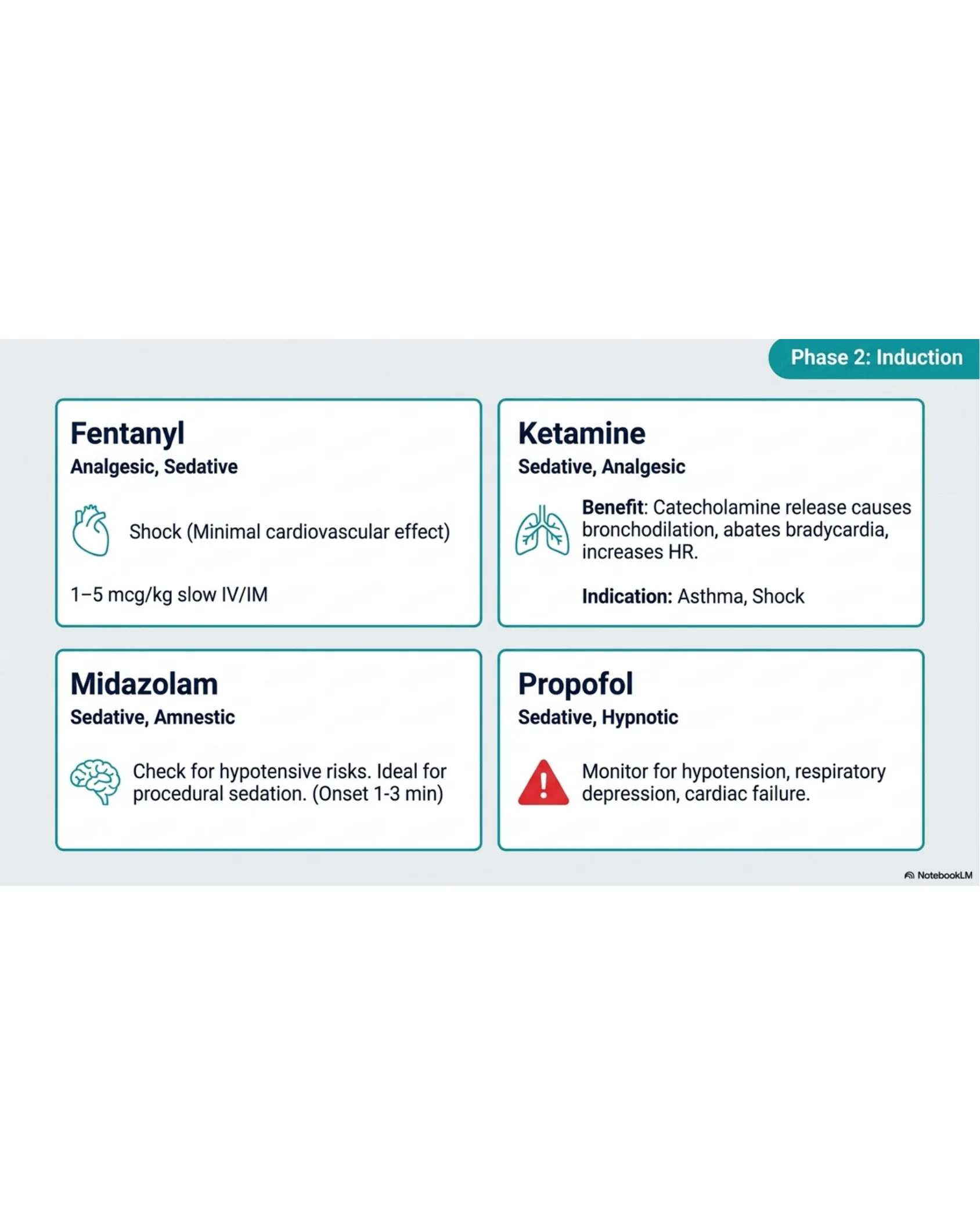
Phase 2: Induction
Fentanyl
Analgesic, Sedative
- Shock (Minimal cardiovascular effect)
- 1–5 mcg/kg slow IV/IM
Ketamine
Sedative, Analgesic
- Benefit: Catecholamine release causes bronchodilation, abates bradycardia, increases HR.
- Indication: Asthma, Shock
Midazolam
Sedative, Amnestic
- Check for hypotensive risks. Ideal for procedural sedation. (Onset 1-3 min)
Propofol
Sedative, Hypnotic
- Monitor for hypotension, respiratory depression, cardiac failure.
Phase 3: Neuromuscular Blockade
Phase 3: Neuromuscular Blockade
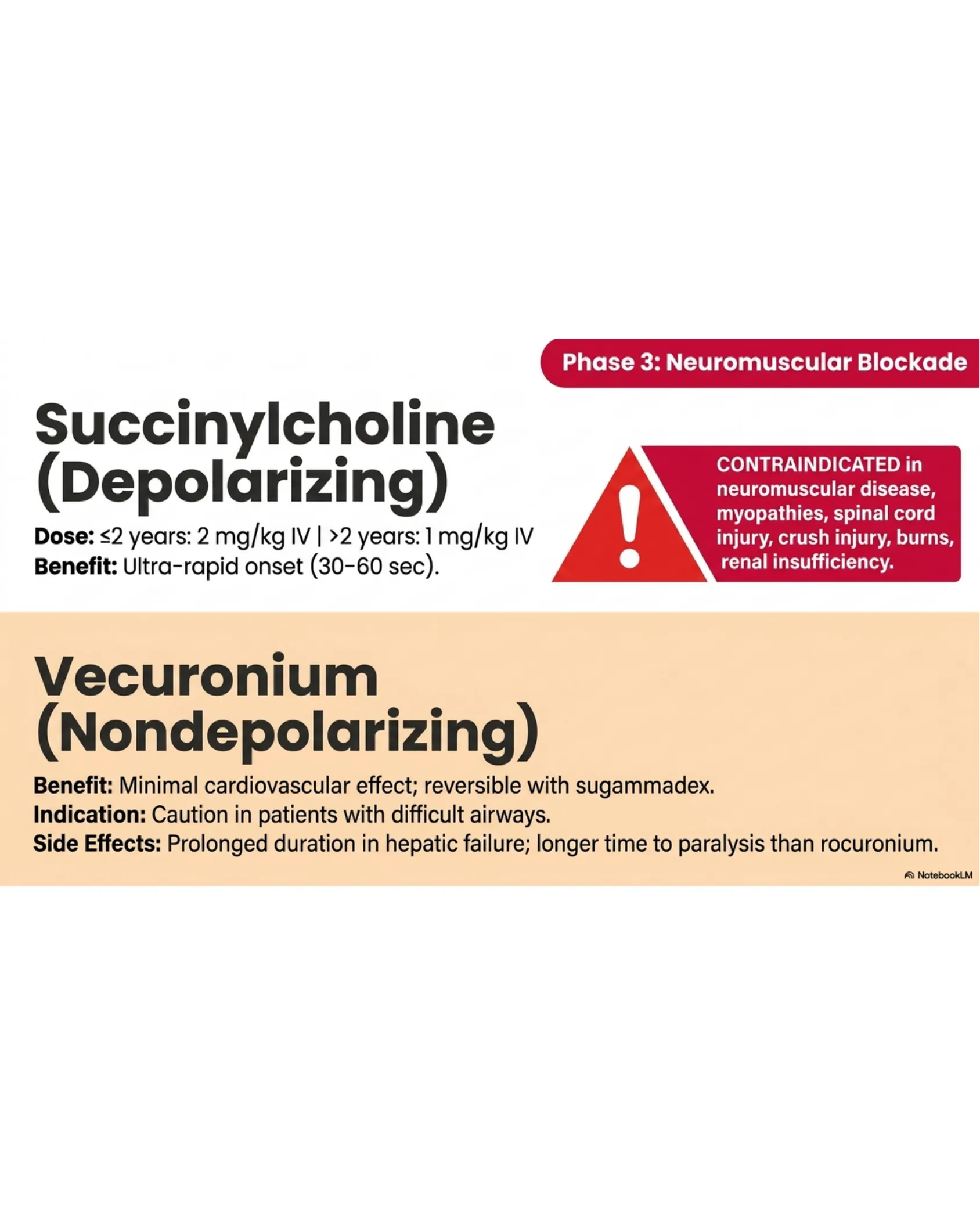
Succinylcholine (Depolarizing)
Dose: ≤2 years: 2 mg/kg IV | >2 years: 1 mg/kg IV
Benefit: Ultra-rapid onset (30-60 sec).
CONTRAINDICATED in neuromuscular disease, myopathies, spinal cord injury, crush injury, burns, renal insufficiency.
Vecuronium (Nondepolarizing)
Benefit: Minimal cardiovascular effect; reversible with sugammadex.
Indication: Caution in patients with difficult airways.
Side Effects: Prolonged duration in hepatic failure; longer time to paralysis than rocuronium.
Rocuronium: The Agent of Choice
Rocuronium: The Agent of Choice
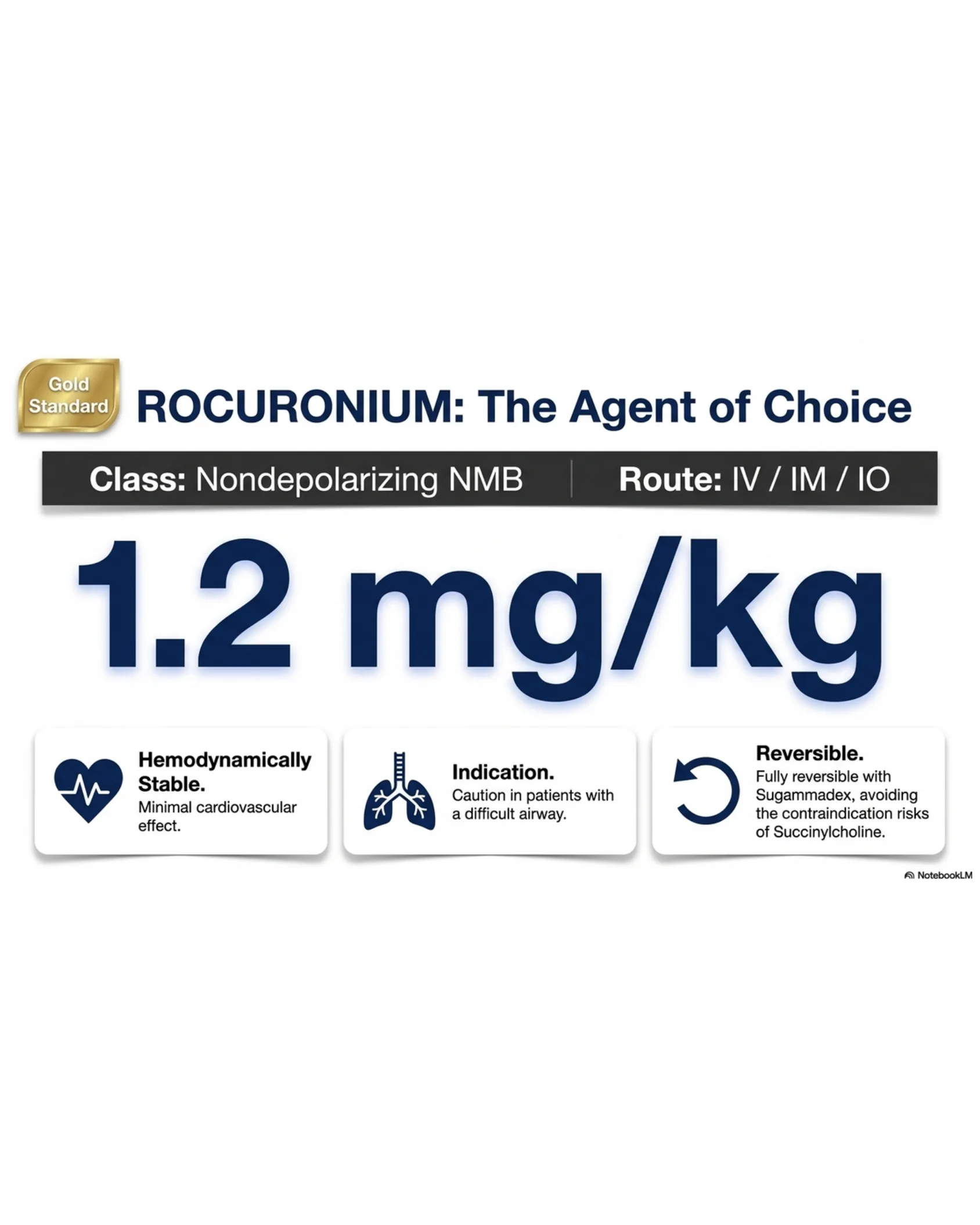
Gold Standard
Class: Nondepolarizing NMB | Route: IV / IM / IO
1.2 mg/kg
- Hemodynamically Stable. Minimal cardiovascular effect.
- Indication. Caution in patients with a difficult airway.
- Reversible. Fully reversible with Sugammadex, avoiding the contraindication risks of Succinylcholine.
Neonatal Airway Algorithm
Neonatal Airway Algorithm
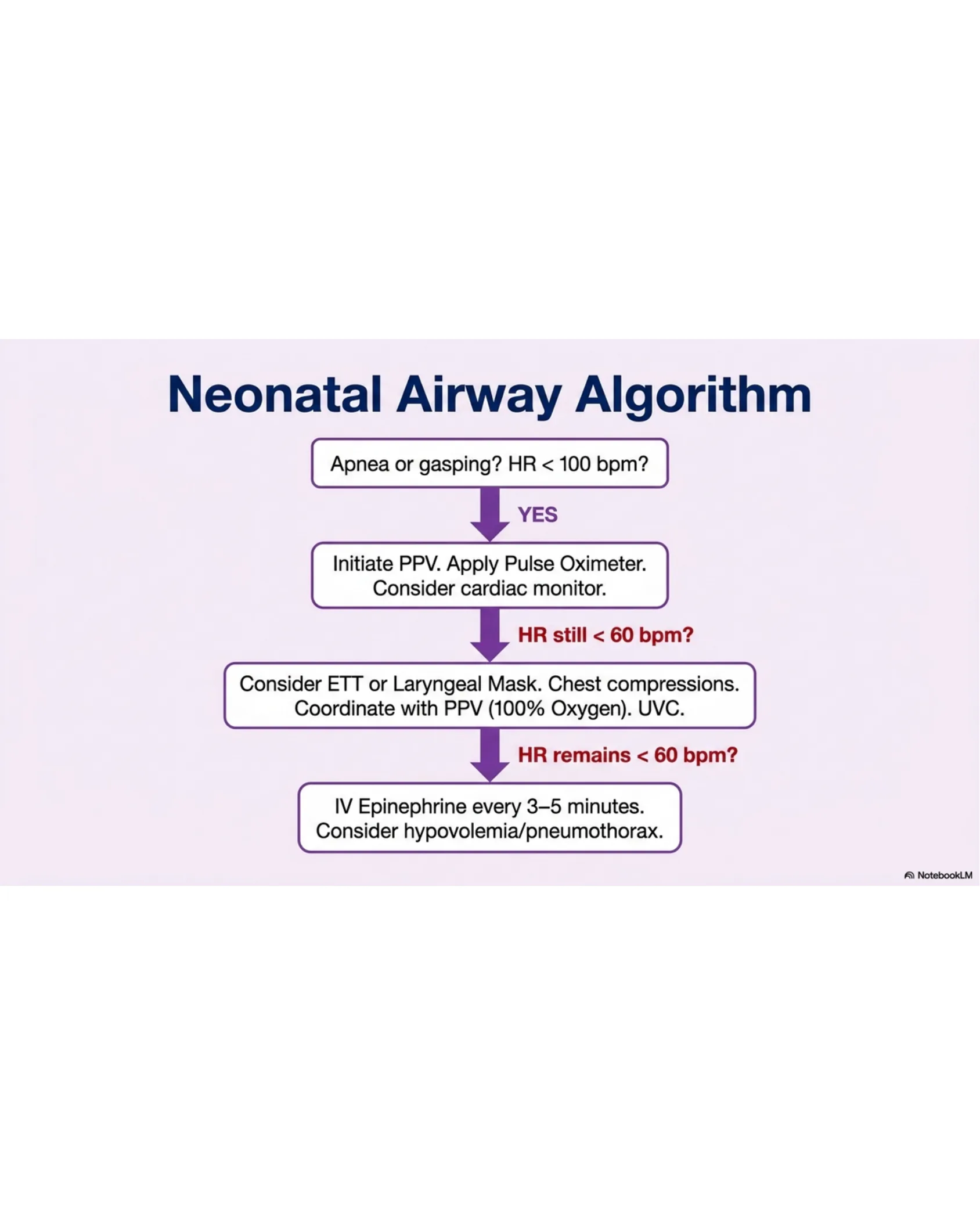
- Apnea or gasping? HR < 100 bpm? — YES
- Initiate PPV. Apply Pulse Oximeter. Consider cardiac monitor. — HR still < 60 bpm?
- Consider ETT or Laryngeal Mask. Chest compressions. Coordinate with PPV (100% Oxygen). UVC. — HR remains < 60 bpm?
- IV Epinephrine every 3–5 minutes. Consider hypovolemia/pneumothorax.
Neonatal Target Metrics
Neonatal Target Metrics
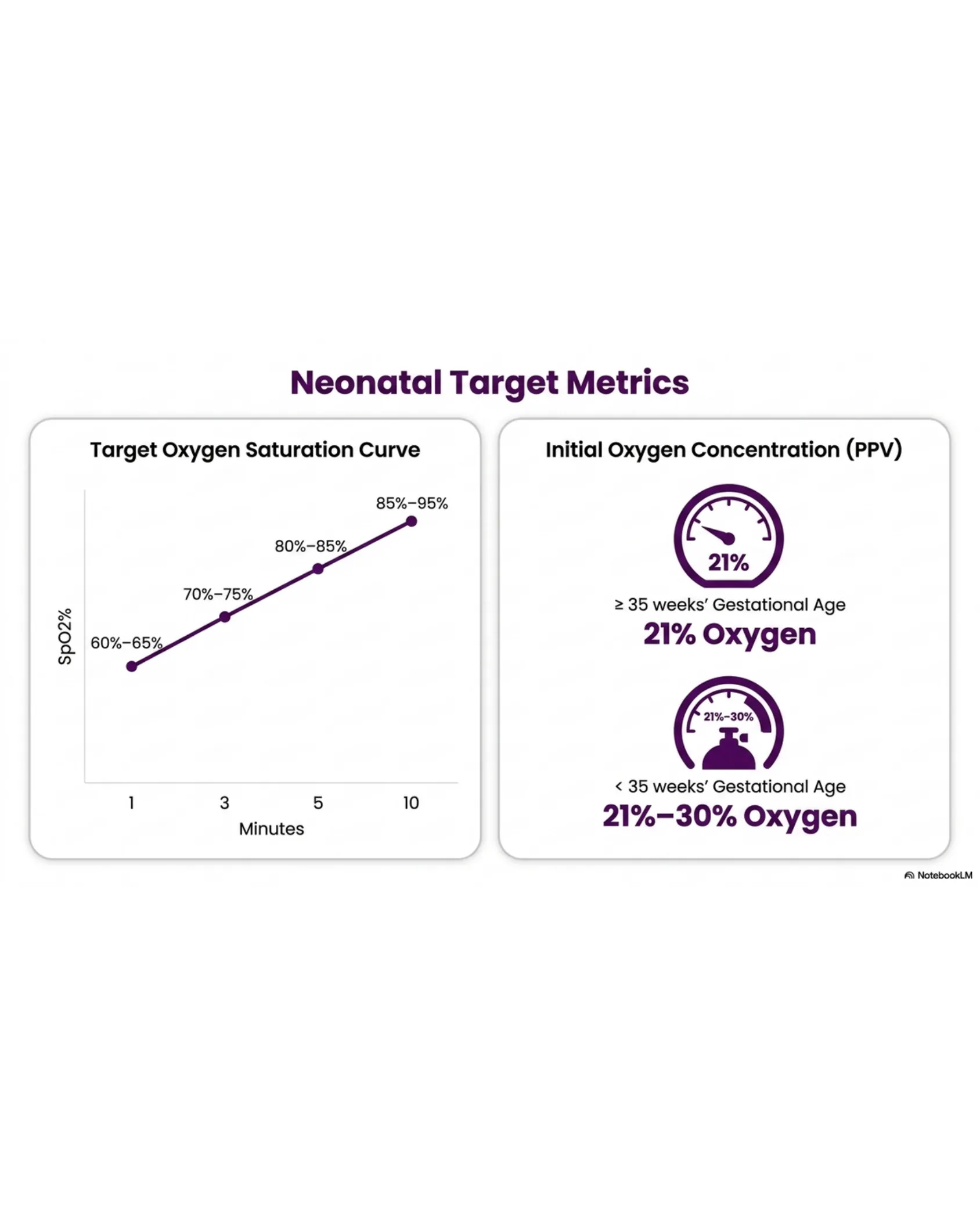
Target Oxygen Saturation Curve
| Minutes | SpO2% |
|---|---|
| 1 | 60%–65% |
| 3 | 70%–75% |
| 5 | 80%–85% |
| 10 | 85%–95% |
Initial Oxygen Concentration (PPV)
- ≥ 35 weeks’ Gestational Age: 21% Oxygen
- < 35 weeks’ Gestational Age: 21%–30% Oxygen
Rescue Pathway: Opioid Reversal
Rescue Pathway: Opioid Reversal
Indications
- Shallow respirations or RR < 8 breaths/min
- Pinpoint pupils
- Unresponsive to physical stimulation
NALOXONE (Narcan)
Dose: 1-2 mcg/kg/dose IV
Administration: Give slowly over 2 minutes.
Titration: Titrate to effect up to a total dose of 10 mcg/kg. If no response, evaluate other causes.
Action shorter than most opioids. Monitor closely; another dose may be required within 30 minutes.