
Intravenous Fluid Therapy in Neonates
Intravenous Fluid Therapy in Neonates
Guideline 2025-28 West Midlands & Digital Bedside Execution via NeoFast.
- Venous hydration
- Continuous medication
- Medicines
- Intubation
- Other calculations and scores
- Procedures
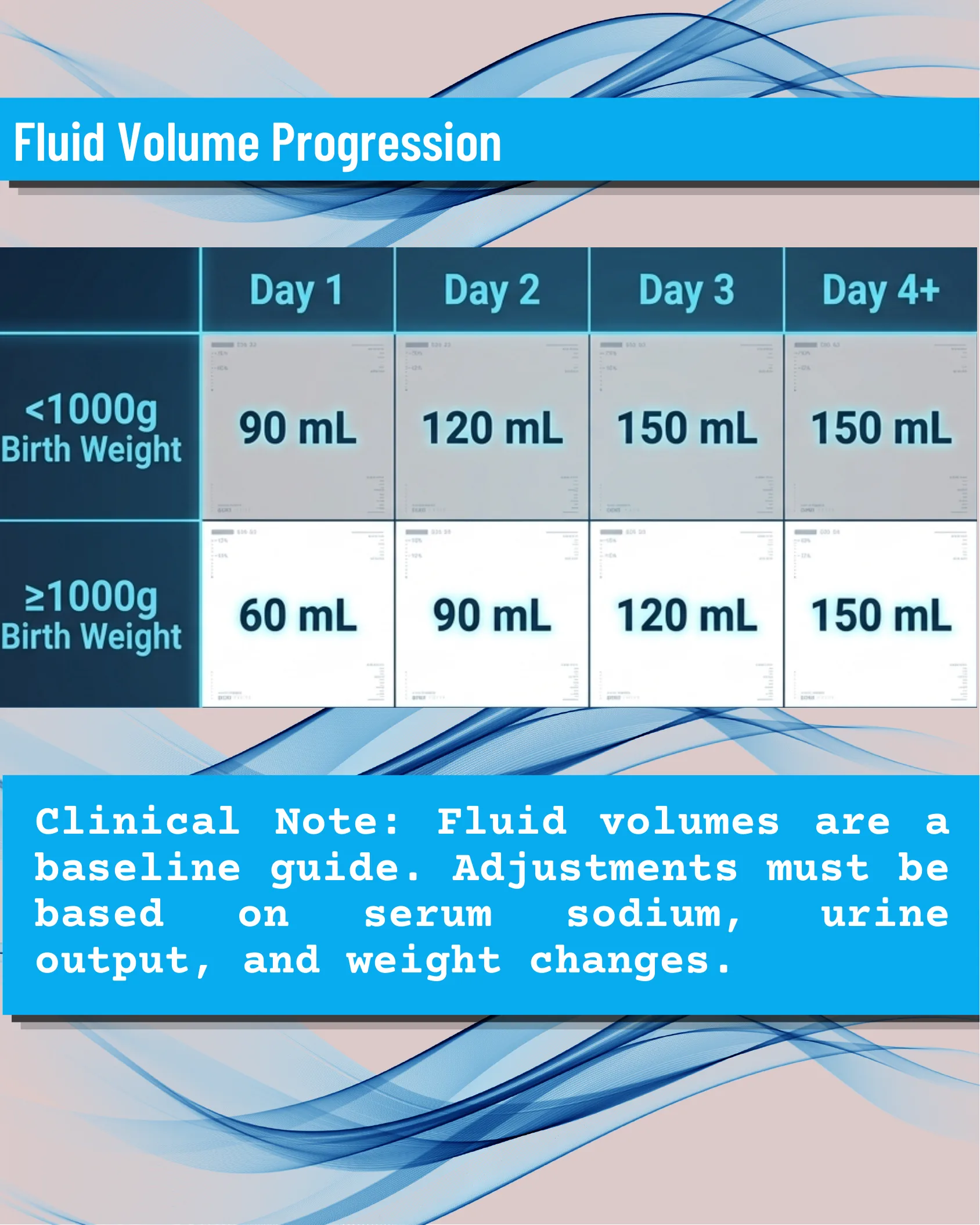
Fluid Volume Progression
Fluid Volume Progression
| Day 1 | Day 2 | Day 3 | Day 4+ | |
|---|---|---|---|---|
| <1000g Birth Weight | 90 mL | 120 mL | 150 mL | 150 mL |
| ≥1000g Birth Weight | 60 mL | 90 mL | 120 mL | 150 mL |
Clinical Note: Fluid volumes are a baseline guide. Adjustments must be based on serum sodium, urine output, and weight changes.
The Physiological Stakes: Fluid Dynamics in the Newborn
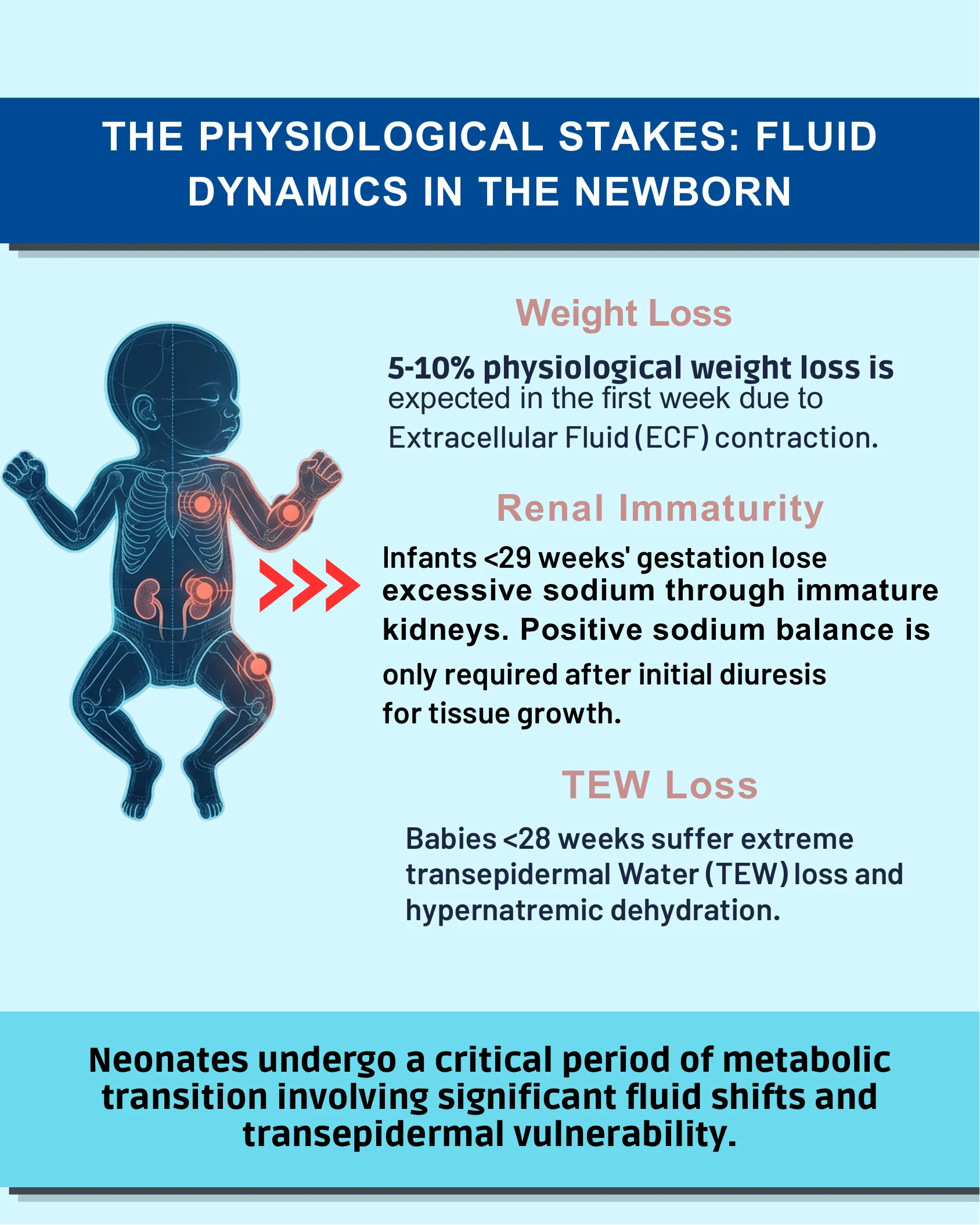
The Physiological Stakes: Fluid Dynamics in the Newborn
- Weight Loss: 5-10% physiological weight loss is expected in the first week due to Extracellular Fluid (ECF) contraction.
- Renal Immaturity: Infants <29 weeks’ gestation lose excessive sodium through immature kidneys. Positive sodium balance is only required after initial diuresis for tissue growth.
- TEW Loss: Babies <28 weeks suffer extreme transepidermal Water (TEW) loss and hypernatremic dehydration.
Neonates undergo a critical period of metabolic transition involving significant fluid shifts and transepidermal vulnerability.
Layering Fluid Composition & Electrolytes / The Glucose Infusion Rate (GIR) Thresholds
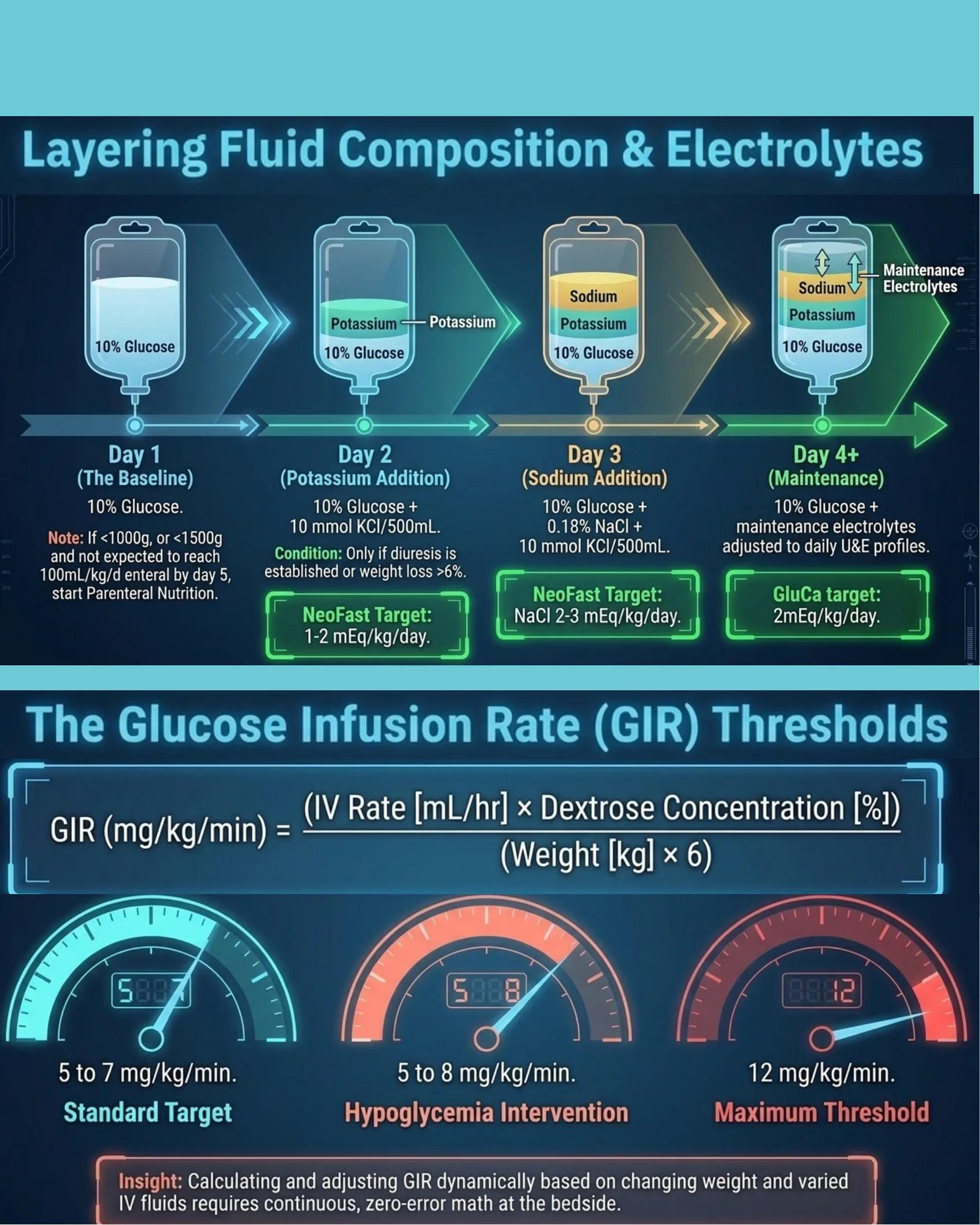
Layering Fluid Composition & Electrolytes
- Day 1 (The Baseline): 10% Glucose.
Note: If <1000g, or <1500g and not expected to reach 100mL/kg/d enteral by day 5, start Parenteral Nutrition. - Day 2 (Potassium Addition): 10% Glucose + 10 mmol KCl/500mL.
Condition: Only if diuresis is established or weight loss >6%.
NeoFast Target: 1-2 mEq/kg/day. - Day 3 (Sodium Addition): 10% Glucose + 0.18% NaCl + 10 mmol KCl/500mL.
NeoFast Target: NaCl 2-3 mEq/kg/day. - Day 4+ (Maintenance): 10% Glucose + maintenance electrolytes adjusted to daily U&E profiles.
GluCa target: 2mEq/kg/day.
The Glucose Infusion Rate (GIR) Thresholds
GIR (mg/kg/min) = (IV Rate [mL/hr] × Dextrose Concentration [%]) / (Weight [kg] × 6)
- Standard Target: 5 to 7 mg/kg/min.
- Hypoglycemia Intervention: 5 to 8 mg/kg/min.
- Maximum Threshold: 12 mg/kg/min.
Insight: Calculating and adjusting GIR dynamically based on changing weight and varied IV fluids requires continuous, zero-error math at the bedside.
Monitoring the Fluid Balance: Serum Creatinine & Urine Output
Monitoring the Fluid Balance
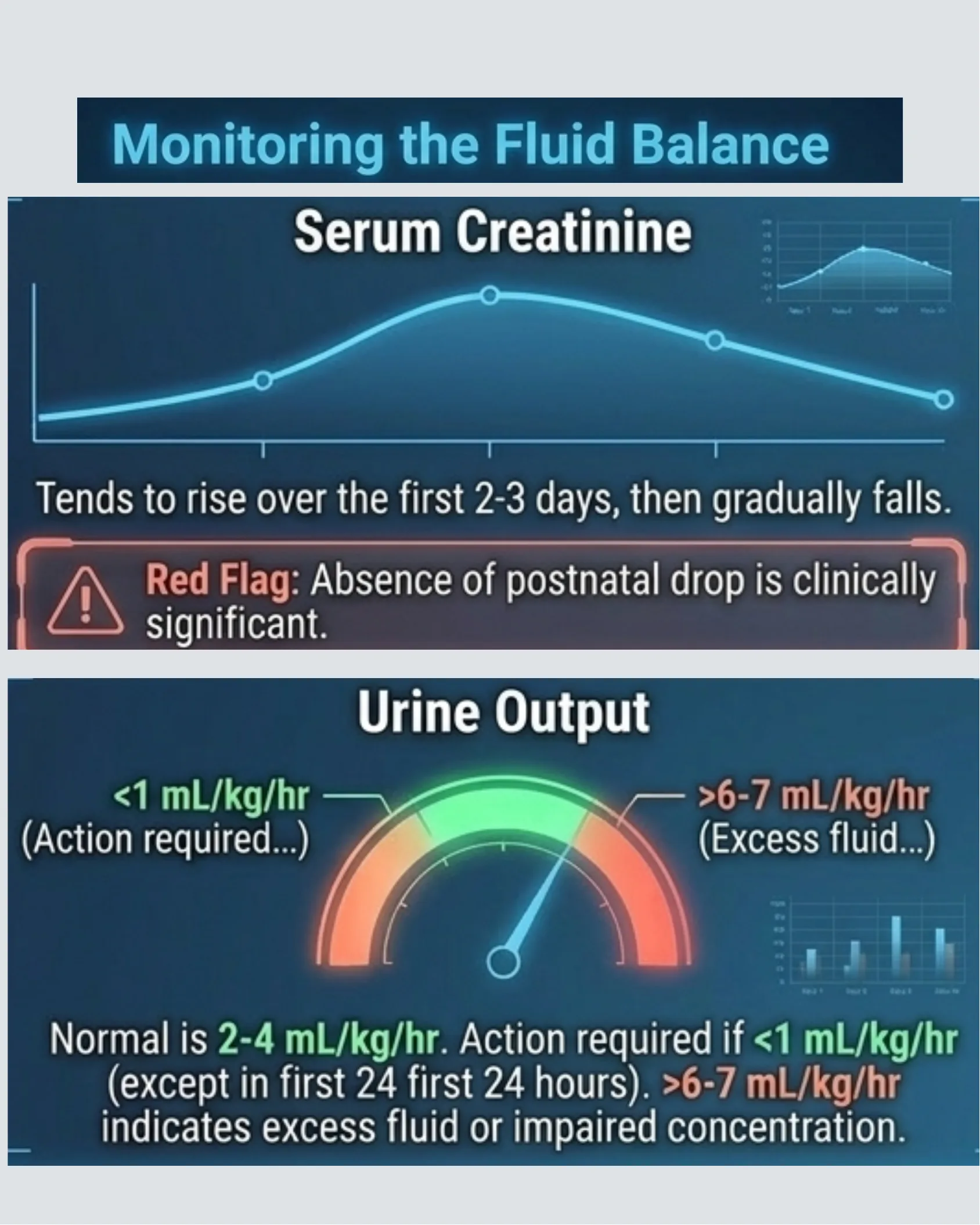
Serum Creatinine
Tends to rise over the first 2-3 days, then gradually falls.
Red Flag: Absence of postnatal drop is clinically significant.
Urine Output
- <1 mL/kg/hr (Action required…)
- >6-7 mL/kg/hr (Excess fluid…)
Normal is 2-4 mL/kg/hr. Action required if <1 mL/kg/hr (except in first 24 hours). >6-7 mL/kg/hr indicates excess fluid or impaired concentration.
Monitoring the Fluid Balance: Serum Sodium & Weight Trends
Monitoring the Fluid Balance
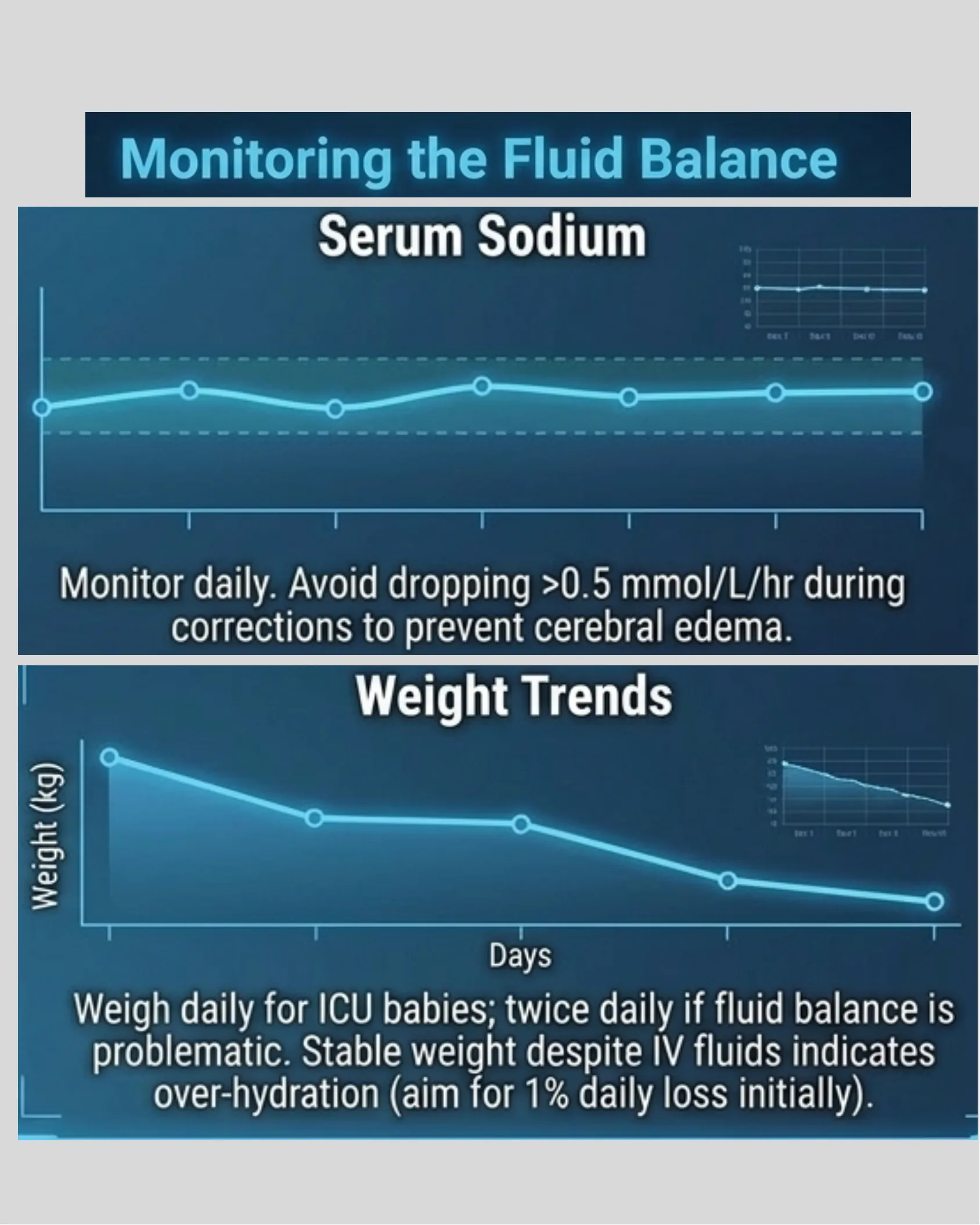
Serum Sodium
Monitor daily. Avoid dropping >0.5 mmol/L/hr during corrections to prevent cerebral edema.
Weight Trends
Weigh daily for ICU babies; twice daily if fluid balance is problematic. Stable weight despite IV fluids indicates over-hydration (aim for 1% daily loss initially).
Troubleshooting Fluid Derangements
Troubleshooting Fluid Derangements
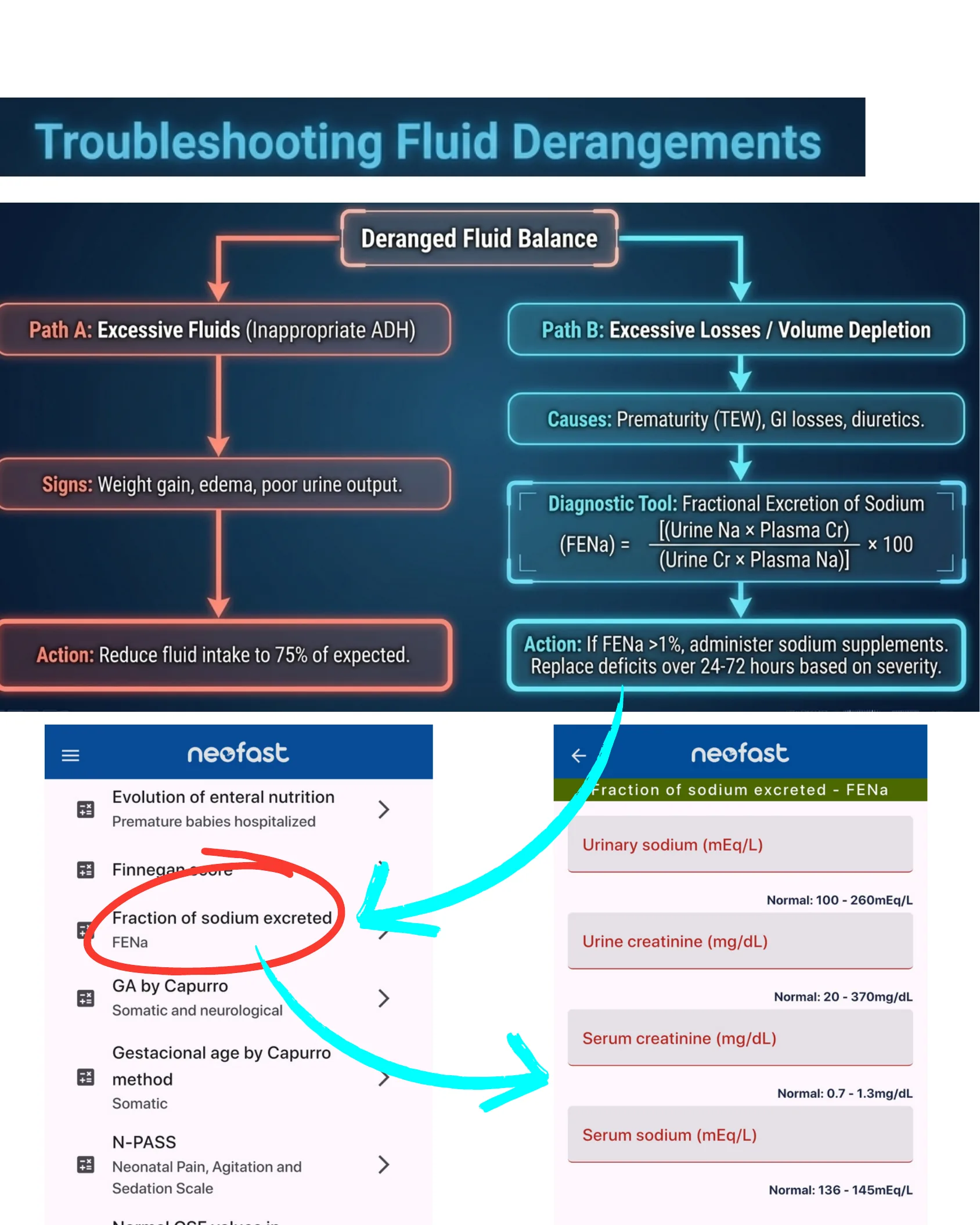
Deranged Fluid Balance
- Path A: Excessive Fluids (Inappropriate ADH)
- Signs: Weight gain, edema, poor urine output.
- Action: Reduce fluid intake to 75% of expected.
- Path B: Excessive Losses / Volume Depletion
- Causes: Prematurity (TEW), GI losses, diuretics.
- Diagnostic Tool: Fractional Excretion of Sodium (FENa) = [(Urine Na × Plasma Cr) / (Urine Cr × Plasma Na)] × 100
- Action: If FENa >1%, administer sodium supplements. Replace deficits over 24-72 hours based on severity.
NeoFast App – FENa Calculator
Menu items shown: Evolution of enteral nutrition (Premature babies hospitalized), Finnegan score, Fraction of sodium excreted – FENa, GA by Capurro (Somatic and neurological), Gestational age by Capurro method (Somatic), N-PASS (Neonatal Pain, Agitation and Sedation Scale), Normal CSF values in…
FENa calculator fields:
- Urinary sodium (mEq/L) — Normal: 100 – 260mEq/L
- Urine creatinine (mg/dL) — Normal: 20 – 370mg/dL
- Serum creatinine (mg/dL) — Normal: 0.7 – 1.3mg/dL
- Serum sodium (mEq/L) — Normal: 136 – 145mEq/L
The Bedside Friction Point
The Bedside Friction Point
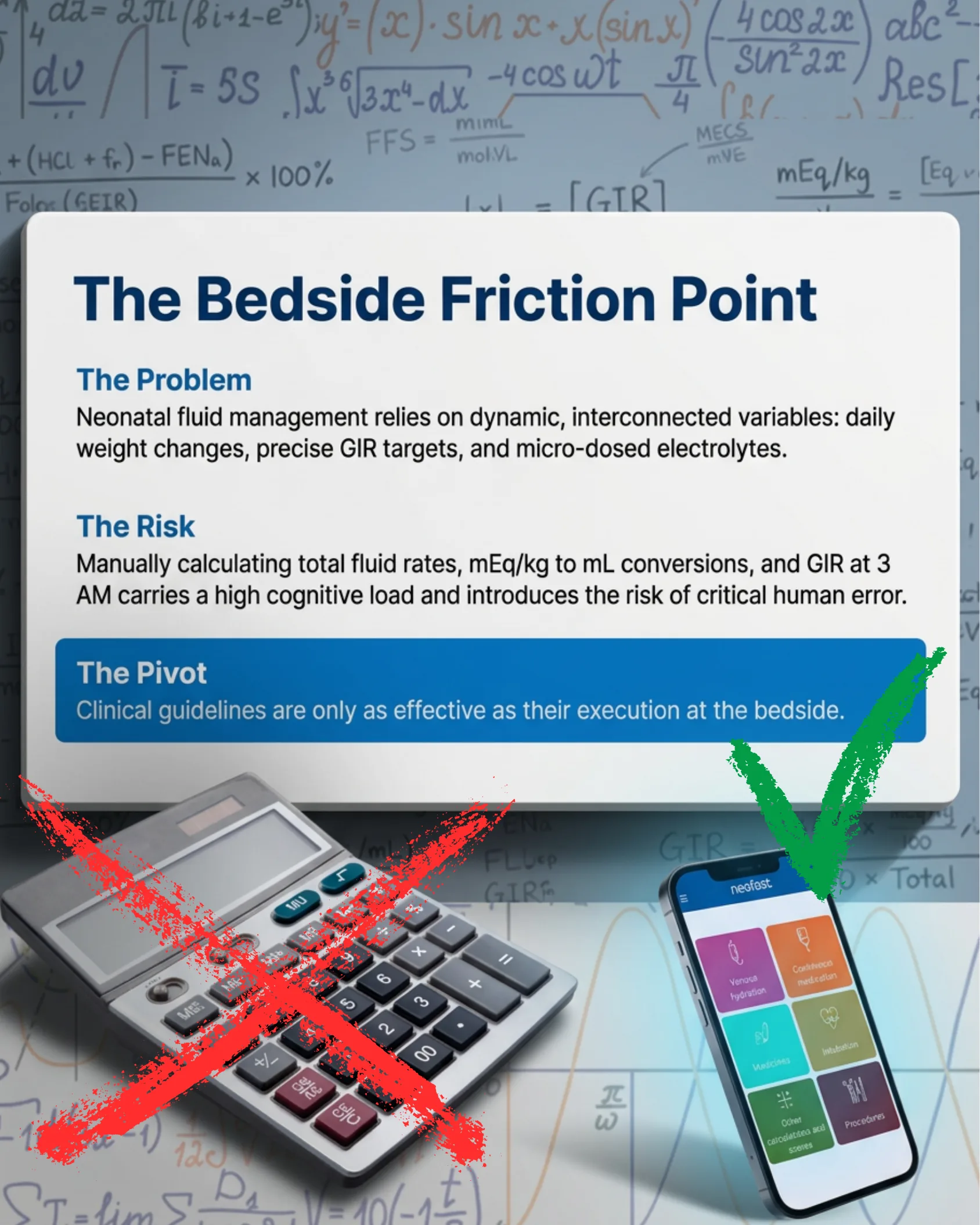
The Problem
Neonatal fluid management relies on dynamic, interconnected variables: daily weight changes, precise GIR targets, and micro-dosed electrolytes.
The Risk
Manually calculating total fluid rates, mEq/kg to mL conversions, and GIR at 3 AM carries a high cognitive load and introduces the risk of critical human error.
The Pivot
Clinical guidelines are only as effective as their execution at the bedside.
- Manual calculator: marked as not recommended.
- NeoFast app: marked as the recommended solution.
The Digital Solution: Instant Precision with NeoFast
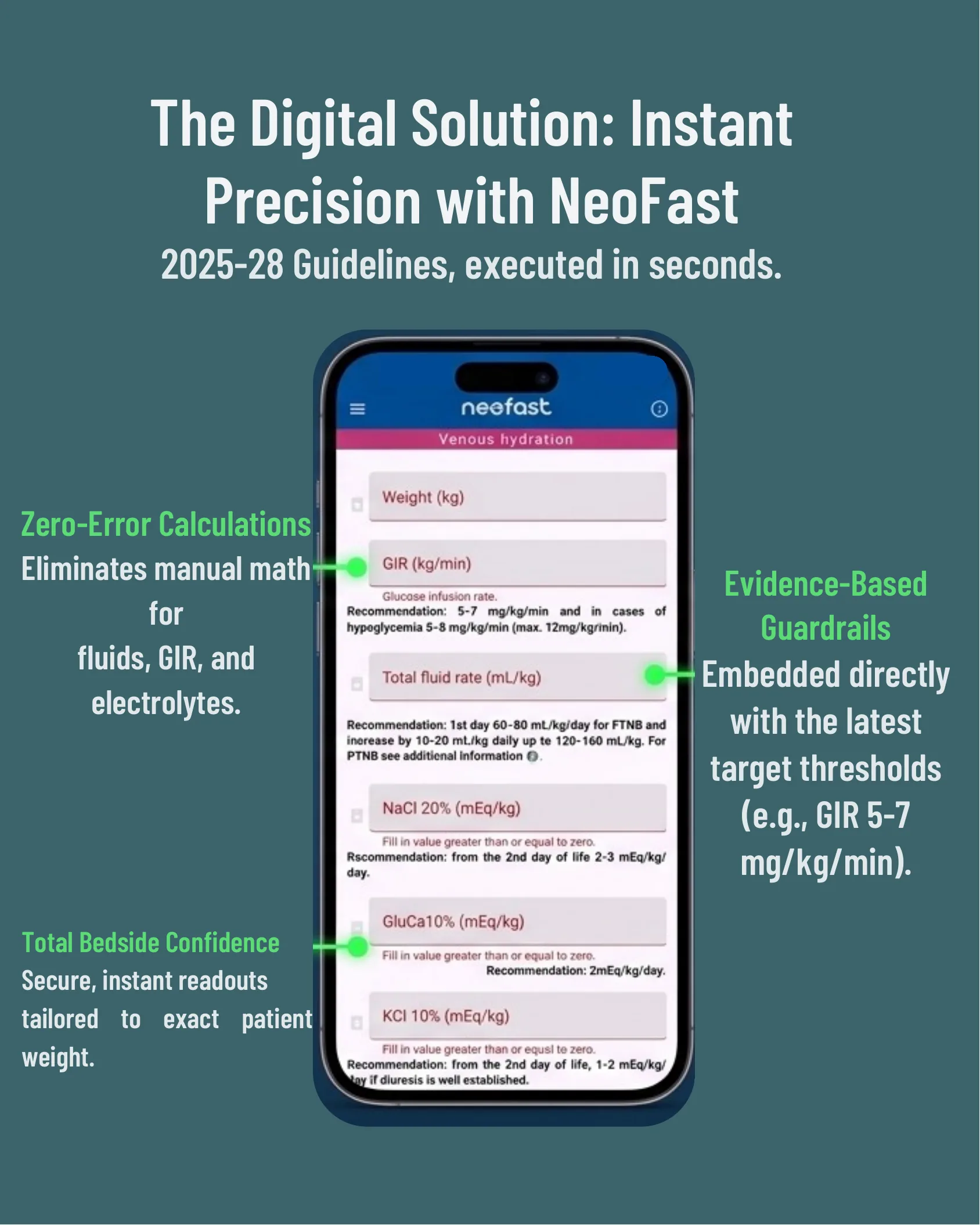
The Digital Solution: Instant Precision with NeoFast
2025-28 Guidelines, executed in seconds.
- Zero-Error Calculations: Eliminates manual math for fluids, GIR, and electrolytes.
- Evidence-Based Guardrails: Embedded directly with the latest target thresholds (e.g., GIR 5-7 mg/kg/min).
- Total Bedside Confidence: Secure, instant readouts tailored to exact patient weight.
App screen fields shown:
- Weight (kg)
- GIR (kg/min) — Glucose infusion rate. Recommendation: 5-7 mg/kg/min and in cases of hypoglycemia 5-8 mg/kg/min (max. 12mg/kg/min).
- Total fluid rate (mL/kg) — Recommendation: 1st day 60-80 mL/kg/day for FTNB and increase by 10-20 mL/kg daily up to 120-160 mL/kg. For PTNB see additional information.
- NaCl 20% (mEq/kg) — Fill in value greater than or equal to zero. Recommendation: from the 2nd day of life 2-3 mEq/kg/day.
- GluCa10% (mEq/kg) — Fill in value greater than or equal to zero. Recommendation: 2mEq/kg/day.
- KCl 10% (mEq/kg) — Fill in value greater than or equal to zero. Recommendation: from the 2nd day of life, 1-2 mEq/kg/day if diuresis is well established.
App Integration: Weight, Fluids & GIR
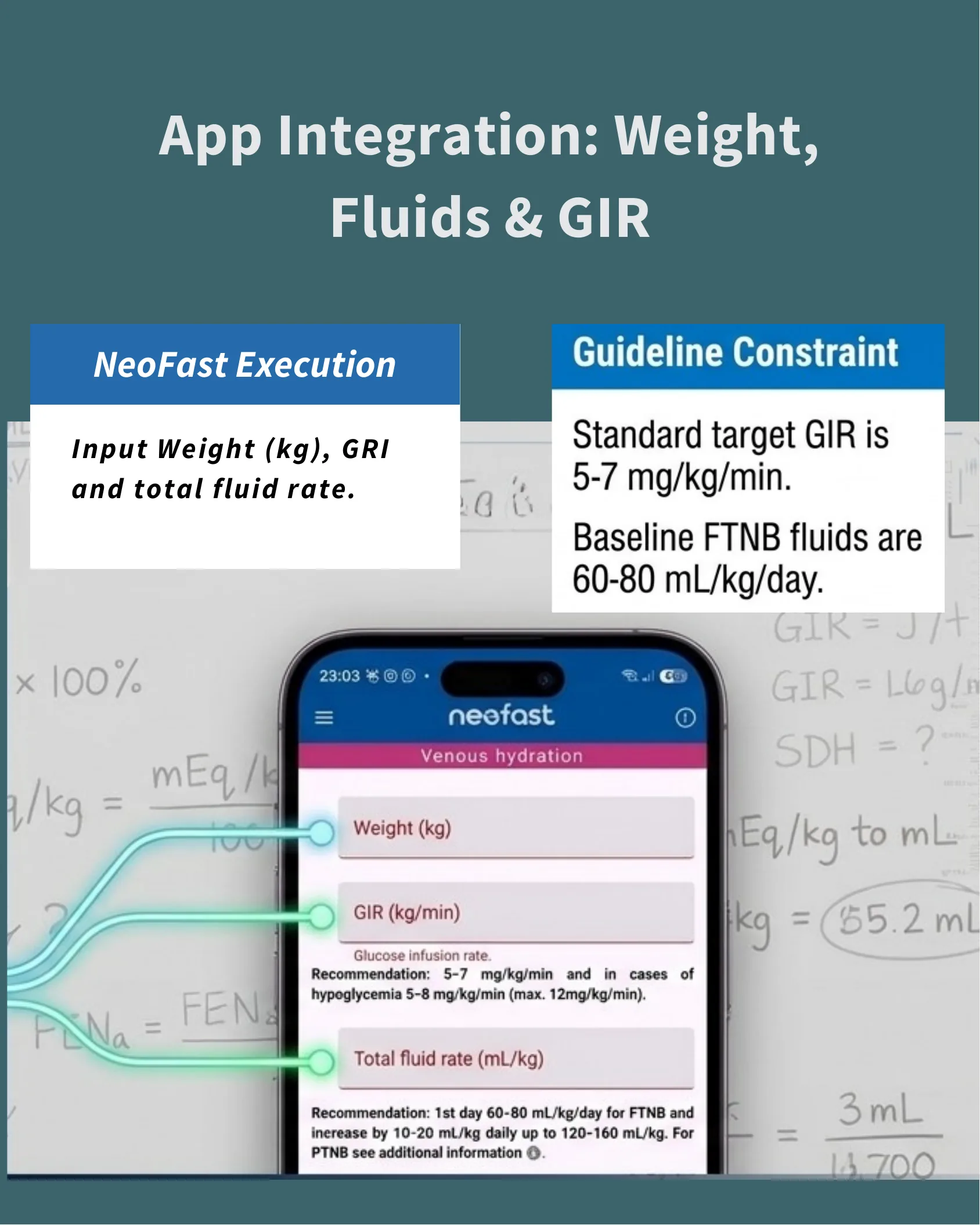
App Integration: Weight, Fluids & GIR
| NeoFast Execution | Guideline Constraint |
|---|---|
| Input Weight (kg), GRI and total fluid rate. | Standard target GIR is 5-7 mg/kg/min. Baseline FTNB fluids are 60-80 mL/kg/day. |
App screen fields highlighted:
- Weight (kg)
- GIR (kg/min) — Glucose infusion rate. Recommendation: 5-7 mg/kg/min and in cases of hypoglycemia 5-8 mg/kg/min (max. 12mg/kg/min).
- Total fluid rate (mL/kg) — Recommendation: 1st day 60-80 mL/kg/day for FTNB and increase by 10-20 mL/kg daily up to 120-160 mL/kg. For PTNB see additional information.
App Integration: Precision Electrolytes & Nutrition
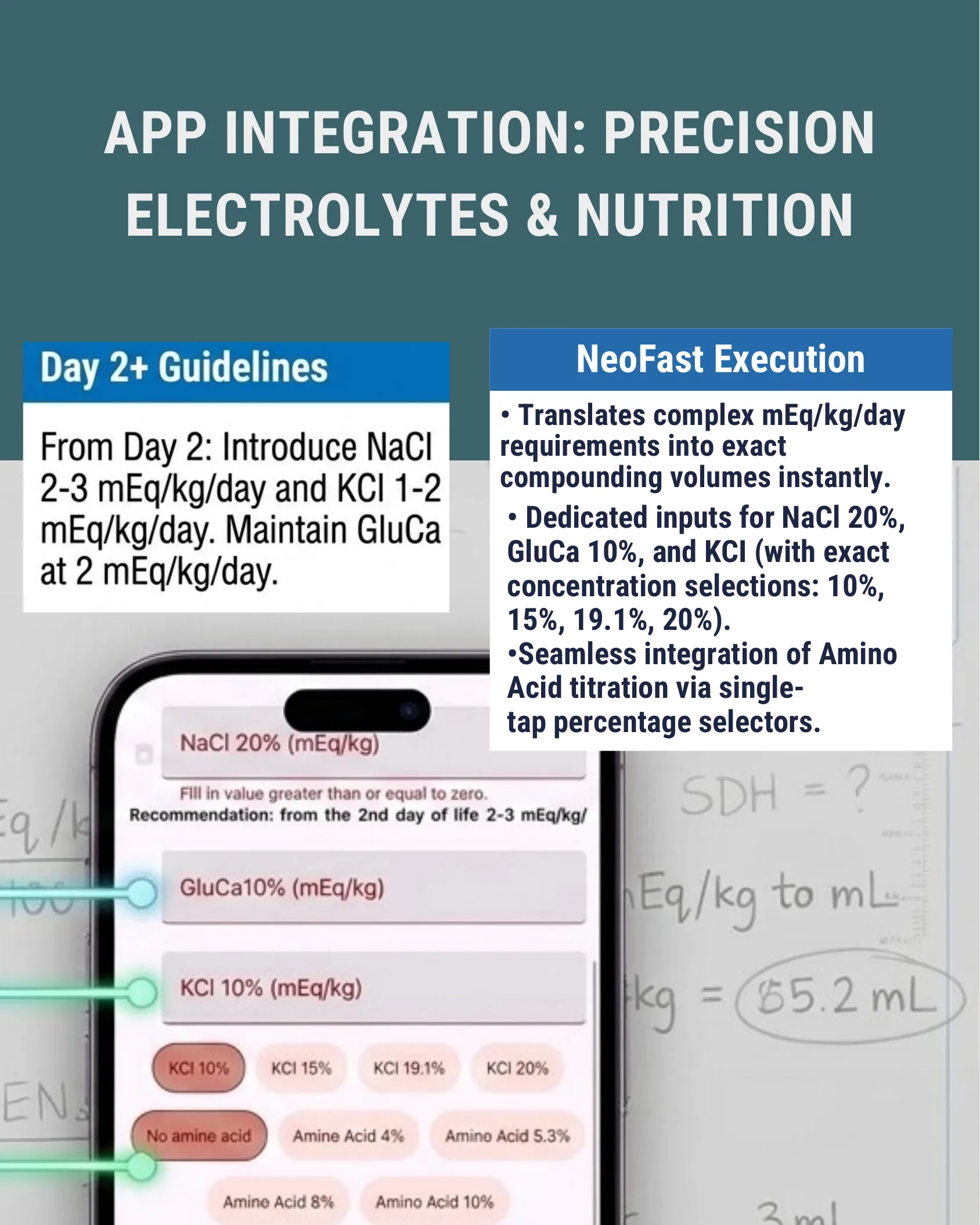
App Integration: Precision Electrolytes & Nutrition
| Day 2+ Guidelines | NeoFast Execution |
|---|---|
| From Day 2: Introduce NaCl 2-3 mEq/kg/day and KCl 1-2 mEq/kg/day. Maintain GluCa at 2 mEq/kg/day. |
|
App screen fields shown:
- NaCl 20% (mEq/kg) — Fill in value greater than or equal to zero. Recommendation: from the 2nd day of life 2-3 mEq/kg/day.
- GluCa10% (mEq/kg)
- KCl 10% (mEq/kg)
Selectable options shown:
- KCl concentrations: KCl 10%, KCl 15%, KCl 19.1%, KCl 20%
- Amino acid options: No amine acid, Amine Acid 4%, Amino Acid 5.3%, Amine Acid 8%, Amino Acid 10%
The Triad of Neonatal Fluid Therapy
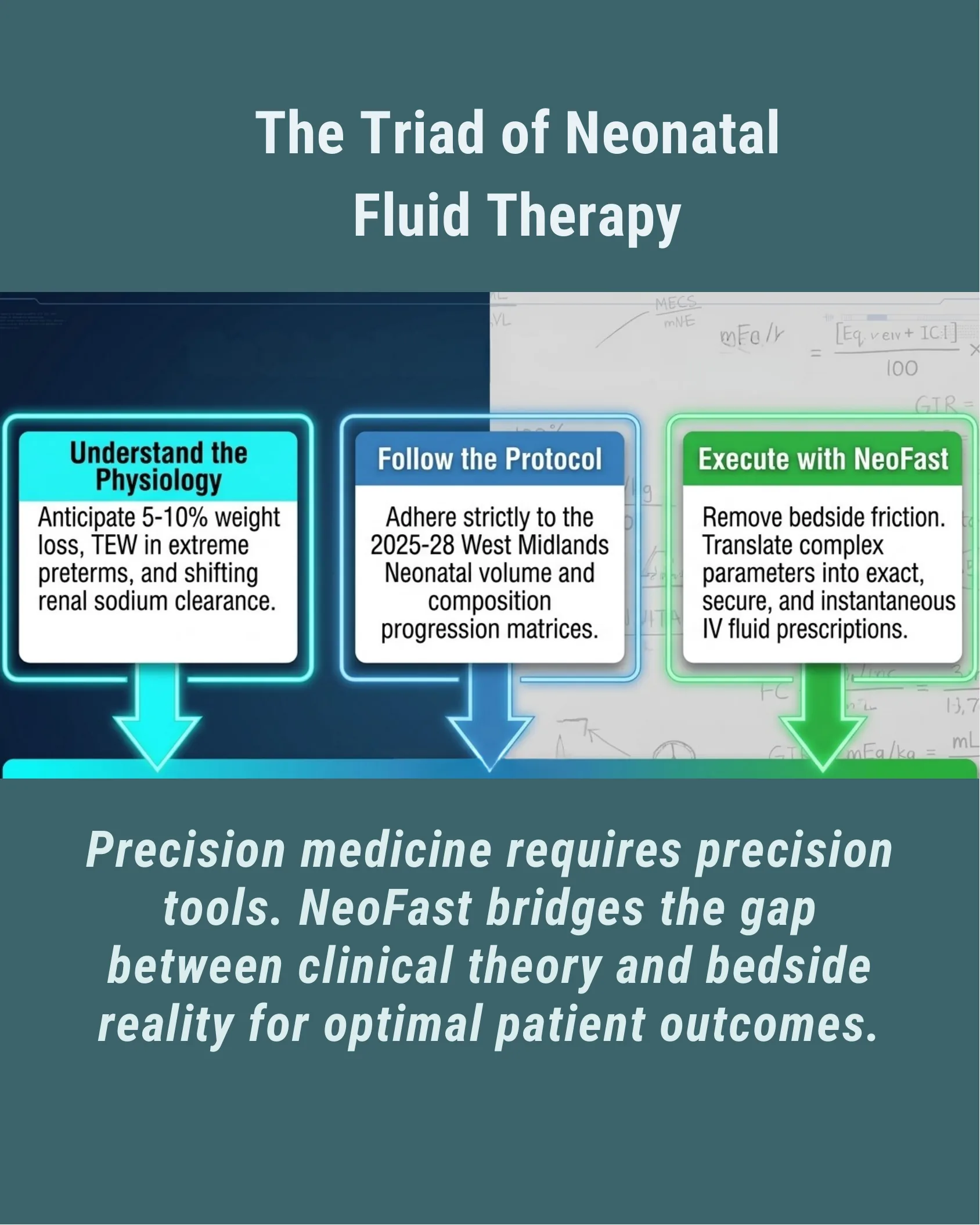
The Triad of Neonatal Fluid Therapy
- Understand the Physiology: Anticipate 5-10% weight loss, TEW in extreme preterms, and shifting renal sodium clearance.
- Follow the Protocol: Adhere strictly to the 2025-28 West Midlands Neonatal volume and composition progression matrices.
- Execute with NeoFast: Remove bedside friction. Translate complex parameters into exact, secure, and instantaneous IV fluid prescriptions.
Precision medicine requires precision tools. NeoFast bridges the gap between clinical theory and bedside reality for optimal patient outcomes.
NeoFast — Global Availability

NeoFast — Worldwide Access
Flags representing countries worldwide surround the NeoFast logo, symbolizing global availability of the app.
- Available on Google Play (Get it on Google Play)
- Available on the App Store (Download on the App Store)
neofast