
Exchange Transfusion in Neonates
Exchange Transfusion in Neonates
Comprehensive Clinical Protocol & Execution Pathway
Indications
Indications
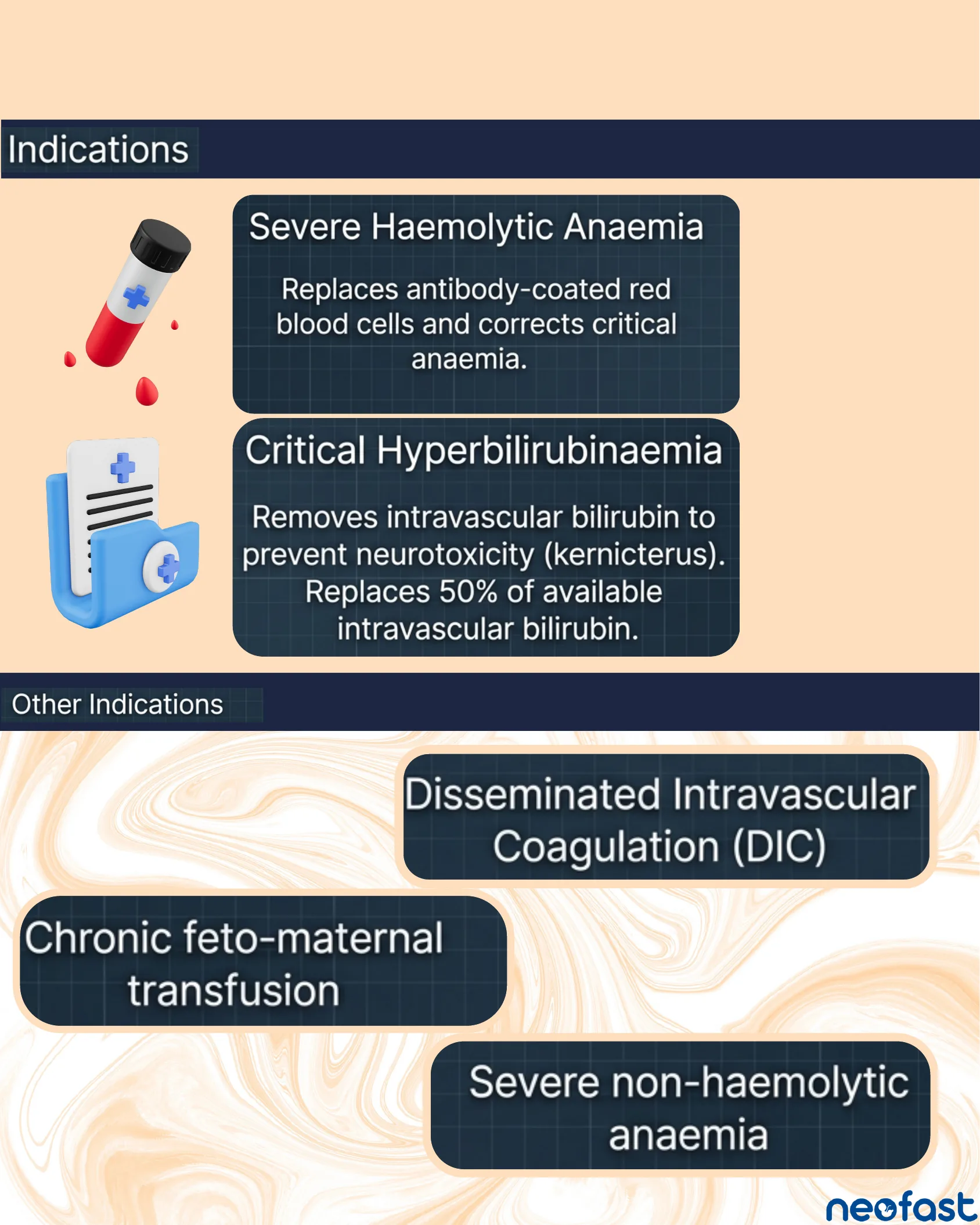
- Severe Haemolytic Anaemia: Replaces antibody-coated red blood cells and corrects critical anaemia.
- Critical Hyperbilirubinaemia: Removes intravascular bilirubin to prevent neurotoxicity (kernicterus). Replaces 50% of available intravascular bilirubin.
Other Indications
- Disseminated Intravascular Coagulation (DIC)
- Chronic feto-maternal transfusion
- Severe non-haemolytic anaemia
Thresholds & Precautions
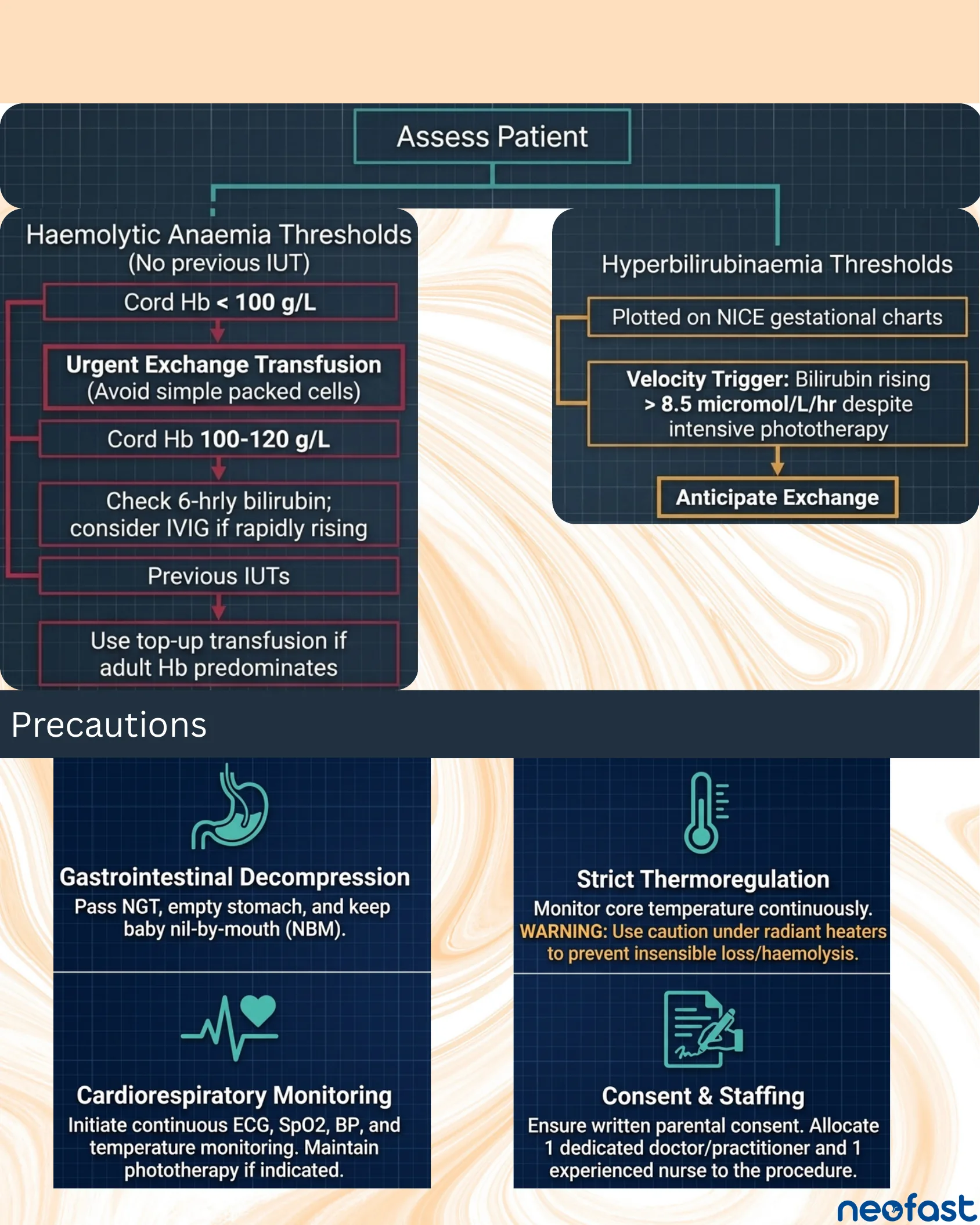
Assess Patient
Haemolytic Anaemia Thresholds (No previous IUT)
- Cord Hb < 100 g/L → Urgent Exchange Transfusion (Avoid simple packed cells)
- Cord Hb 100-120 g/L → Check 6-hrly bilirubin; consider IVIG if rapidly rising
- Previous IUTs → Use top-up transfusion if adult Hb predominates
Hyperbilirubinaemia Thresholds
- Plotted on NICE gestational charts
- Velocity Trigger: Bilirubin rising > 8.5 micromol/L/hr despite intensive phototherapy
- → Anticipate Exchange
Precautions
- Gastrointestinal Decompression: Pass NGT, empty stomach, and keep baby nil-by-mouth (NBM).
- Strict Thermoregulation: Monitor core temperature continuously. WARNING: Use caution under radiant heaters to prevent insensible loss/haemolysis.
- Cardiorespiratory Monitoring: Initiate continuous ECG, SpO2, BP, and temperature monitoring. Maintain phototherapy if indicated.
- Consent & Staffing: Ensure written parental consent. Allocate 1 dedicated doctor/practitioner and 1 experienced nurse to the procedure.
Characteristics of the Blood to be Requested
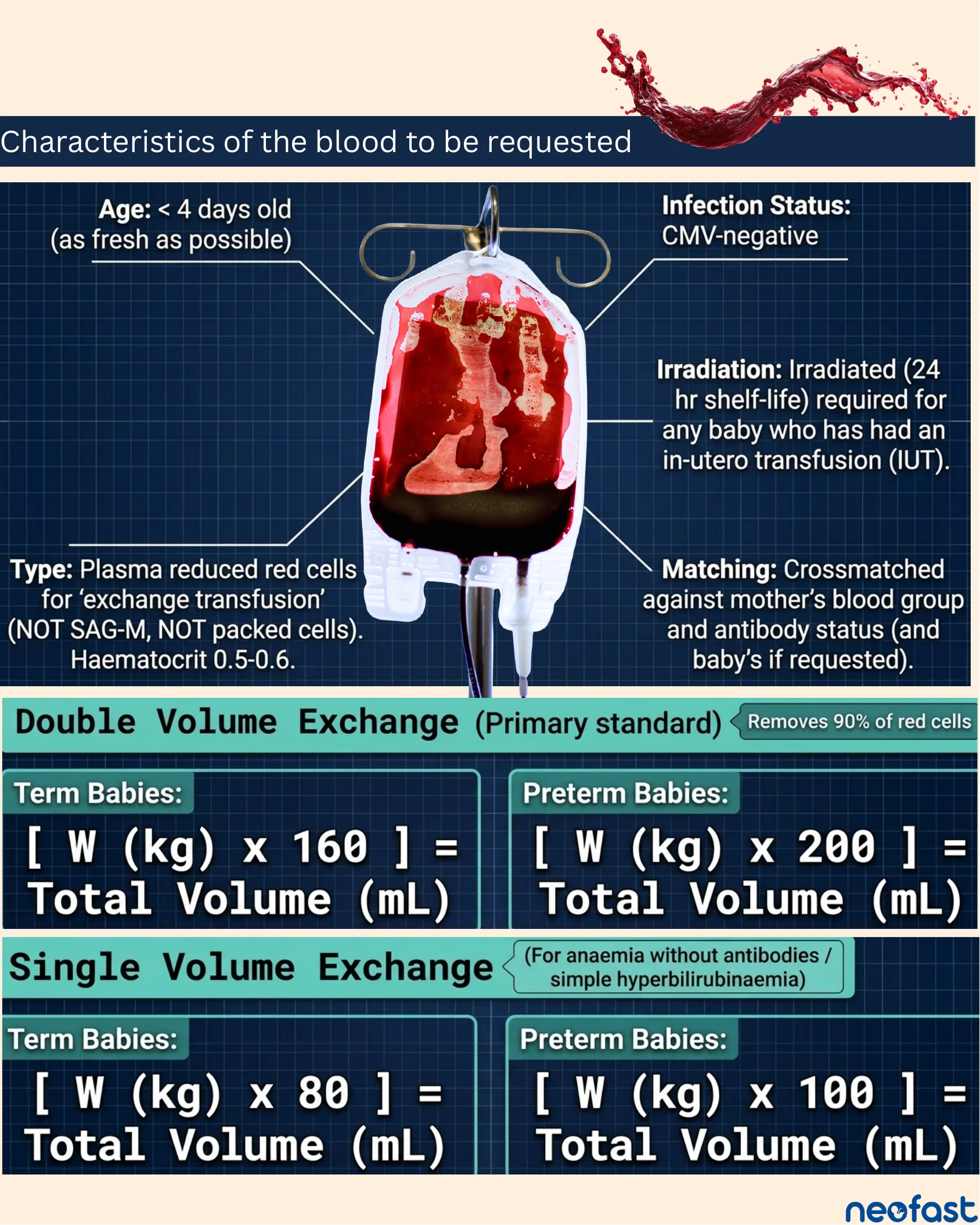
Characteristics of the blood to be requested
- Age: < 4 days old (as fresh as possible)
- Infection Status: CMV-negative
- Type: Plasma reduced red cells for ‘exchange transfusion’ (NOT SAG-M, NOT packed cells). Haematocrit 0.5-0.6.
- Irradiation: Irradiated (24 hr shelf-life) required for any baby who has had an in-utero transfusion (IUT).
- Matching: Crossmatched against mother’s blood group and antibody status (and baby’s if requested).
Double Volume Exchange (Primary standard) – Removes 90% of red cells
- Term Babies: [W (kg) x 160] = Total Volume (mL)
- Preterm Babies: [W (kg) x 200] = Total Volume (mL)
Single Volume Exchange (For anaemia without antibodies / simple hyperbilirubinaemia)
- Term Babies: [W (kg) x 80] = Total Volume (mL)
- Preterm Babies: [W (kg) x 100] = Total Volume (mL)
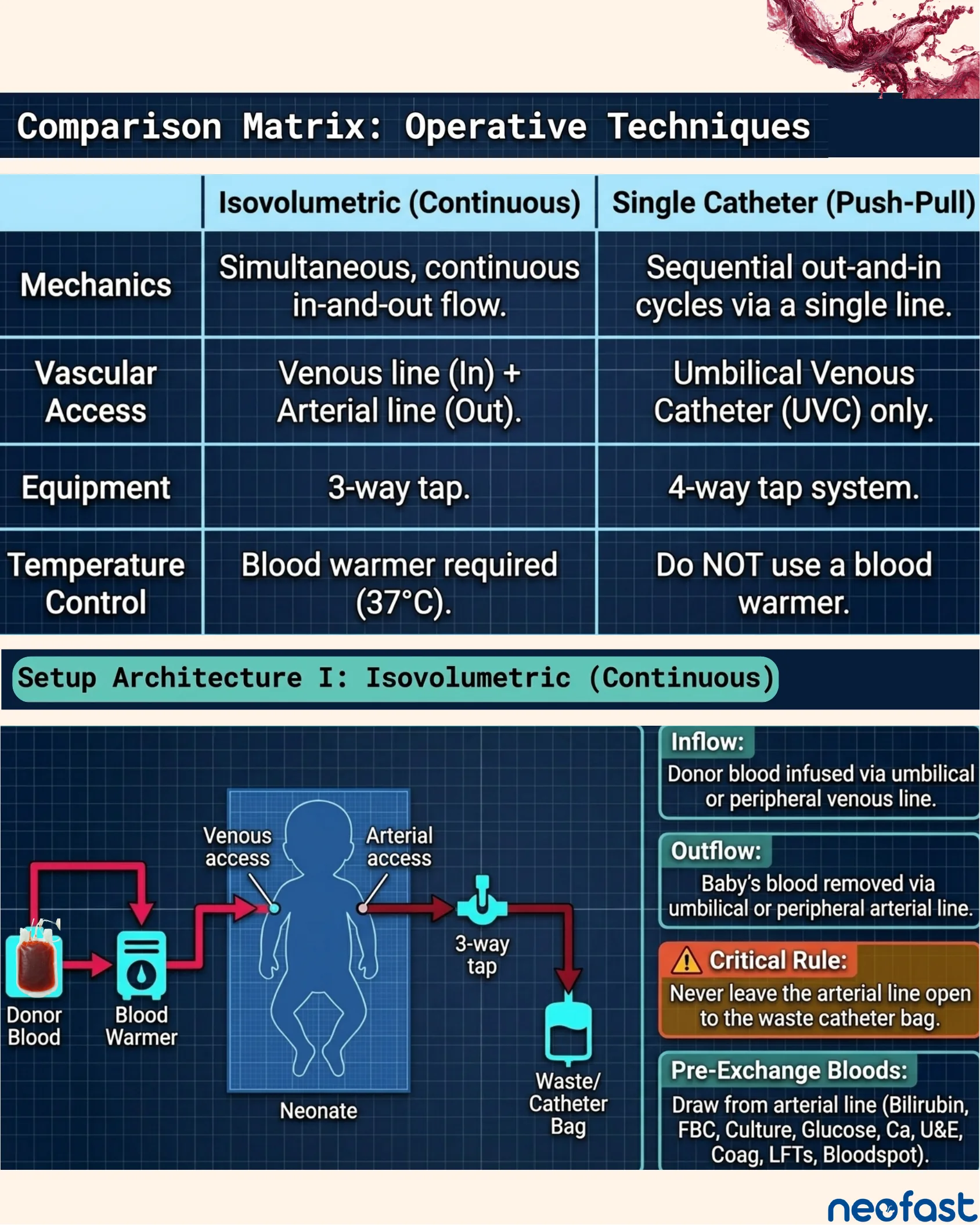
Comparison Matrix: Operative Techniques
Comparison Matrix: Operative Techniques
| Isovolumetric (Continuous) | Single Catheter (Push-Pull) | |
|---|---|---|
| Mechanics | Simultaneous, continuous in-and-out flow. | Sequential out-and-in cycles via a single line. |
| Vascular Access | Venous line (In) + Arterial line (Out). | Umbilical Venous Catheter (UVC) only. |
| Equipment | 3-way tap. | 4-way tap system. |
| Temperature Control | Blood warmer required (37°C). | Do NOT use a blood warmer. |
Setup Architecture I: Isovolumetric (Continuous)
- Inflow: Donor blood infused via umbilical or peripheral venous line.
- Outflow: Baby’s blood removed via umbilical or peripheral arterial line.
- Critical Rule: Never leave the arterial line open to the waste catheter bag.
- Pre-Exchange Bloods: Draw from arterial line (Bilirubin, FBC, Culture, Glucose, Ca, U&E, Coag, LFTs, Bloodspot).
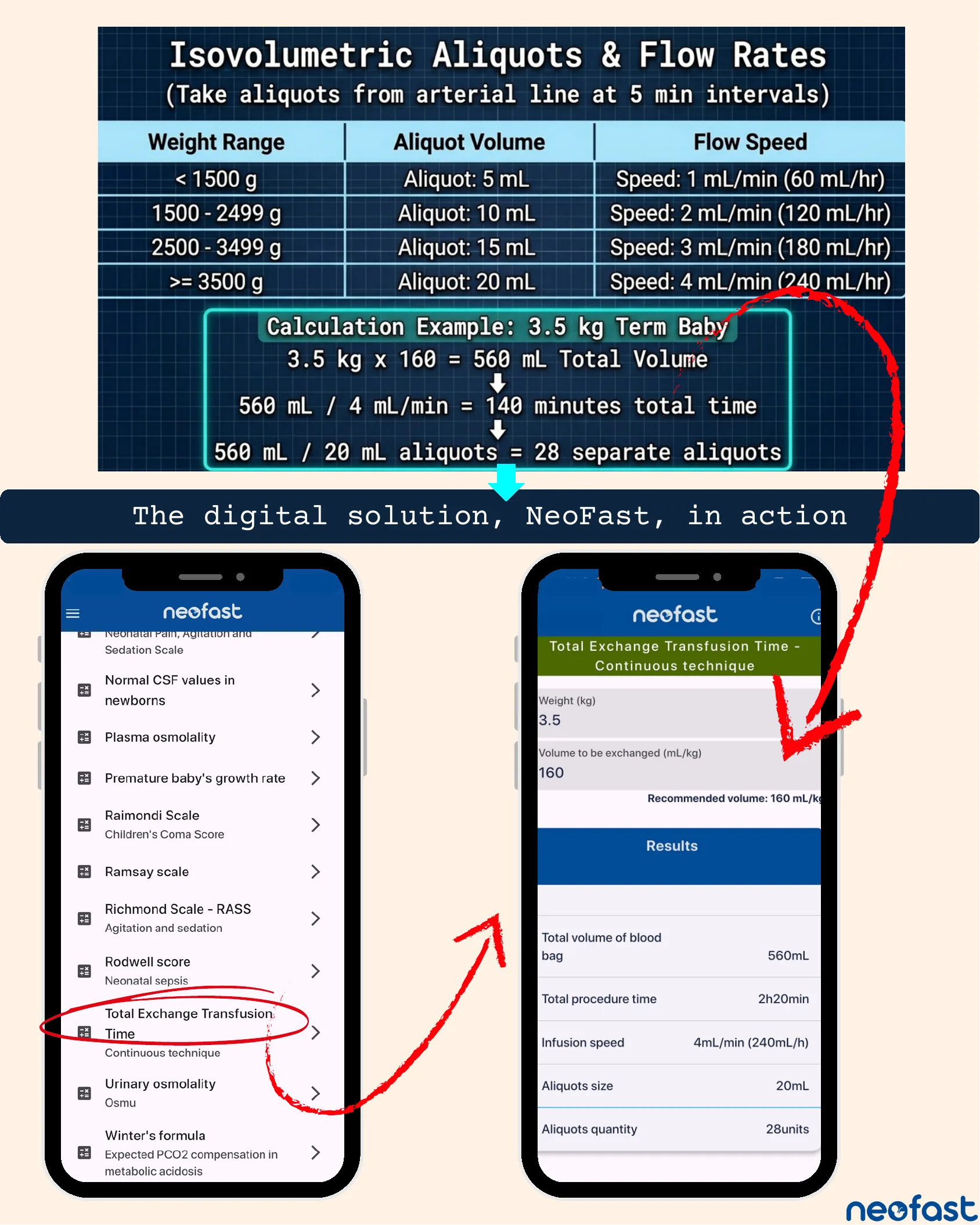
Isovolumetric Aliquots & Flow Rates
Isovolumetric Aliquots & Flow Rates
(Take aliquots from arterial line at 5 min intervals)
| Weight Range | Aliquot Volume | Flow Speed |
|---|---|---|
| < 1500 g | Aliquot: 5 mL | Speed: 1 mL/min (60 mL/hr) |
| 1500 – 2499 g | Aliquot: 10 mL | Speed: 2 mL/min (120 mL/hr) |
| 2500 – 3499 g | Aliquot: 15 mL | Speed: 3 mL/min (180 mL/hr) |
| >= 3500 g | Aliquot: 20 mL | Speed: 4 mL/min (240 mL/hr) |
Calculation Example: 3.5 kg Term Baby
- 3.5 kg x 160 = 560 mL Total Volume
- 560 mL / 4 mL/min = 140 minutes total time
- 560 mL / 20 mL aliquots = 28 separate aliquots
The digital solution, NeoFast, in action
App screenshot: Total Exchange Transfusion Time – Continuous technique
- Weight (kg): 3.5
- Volume to be exchanged (mL/kg): 160 (Recommended volume: 160 mL/kg)
Results:
- Total volume of blood bag: 560mL
- Total procedure time: 2h20min
- Infusion speed: 4mL/min (240mL/h)
- Aliquots size: 20mL
- Aliquots quantity: 28units
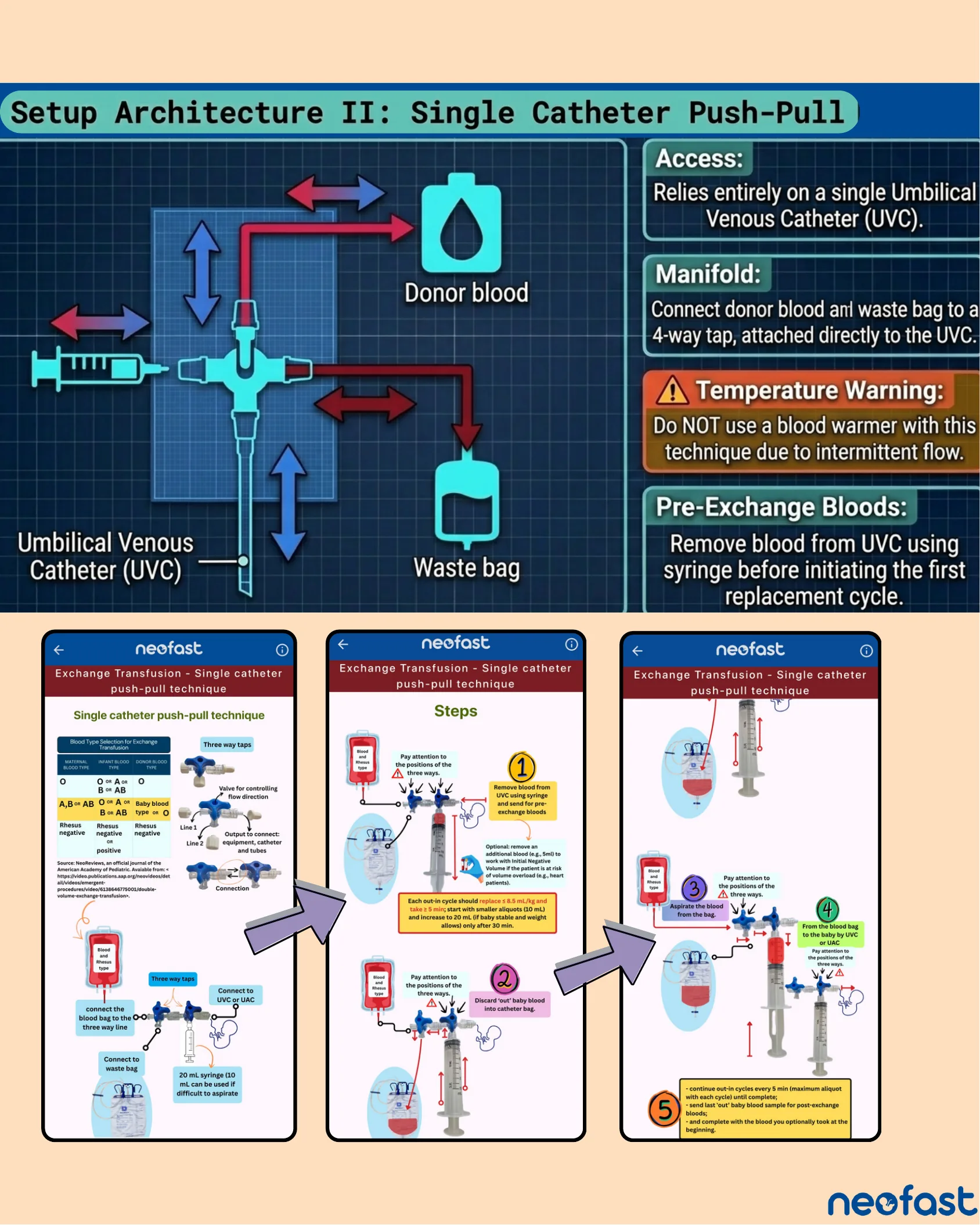
Setup Architecture II: Single Catheter Push-Pull
Setup Architecture II: Single Catheter Push-Pull
- Access: Relies entirely on a single Umbilical Venous Catheter (UVC).
- Manifold: Connect donor blood and waste bag to a 4-way tap, attached directly to the UVC.
- Temperature Warning: Do NOT use a blood warmer with this technique due to intermittent flow.
- Pre-Exchange Bloods: Remove blood from UVC using syringe before initiating the first replacement cycle.
App Screenshots: Single catheter push-pull technique
Blood Type Selection for Exchange Transfusion:
| Maternal Blood Type | Infant Blood Type | Donor Blood Type |
|---|---|---|
| O | O or A or B or AB | O |
| A, B or AB | O or A or B or AB | Baby blood type or O |
| Rhesus negative | Rhesus negative or positive | Rhesus negative |
Source: NeoReviews, an official journal of the American Academy of Pediatric.
Steps
- Remove blood from UVC using syringe and send for pre-exchange bloods. (Optional: remove an additional blood (e.g., 5ml) to work with Initial Negative Volume if the patient is at risk of volume overload, e.g., heart patients.) Each out-in cycle should replace ≤ 8.5 mL/kg and take ≥ 5 min; start with smaller aliquots (10 mL) and increase to 20 mL (if baby stable and weight allows) only after 30 min.
- Discard ‘out’ baby blood into catheter bag.
- Aspirate the blood from the bag.
- From the blood bag to the baby by UVC or UAC.
- Continue out-in cycles every 5 min (maximum aliquot with each cycle) until complete; send last ‘out’ baby blood sample for post-exchange bloods; and complete with the blood you optionally took at the beginning.
Execution: The Push-Pull Cycle & Intra-Operative Monitoring
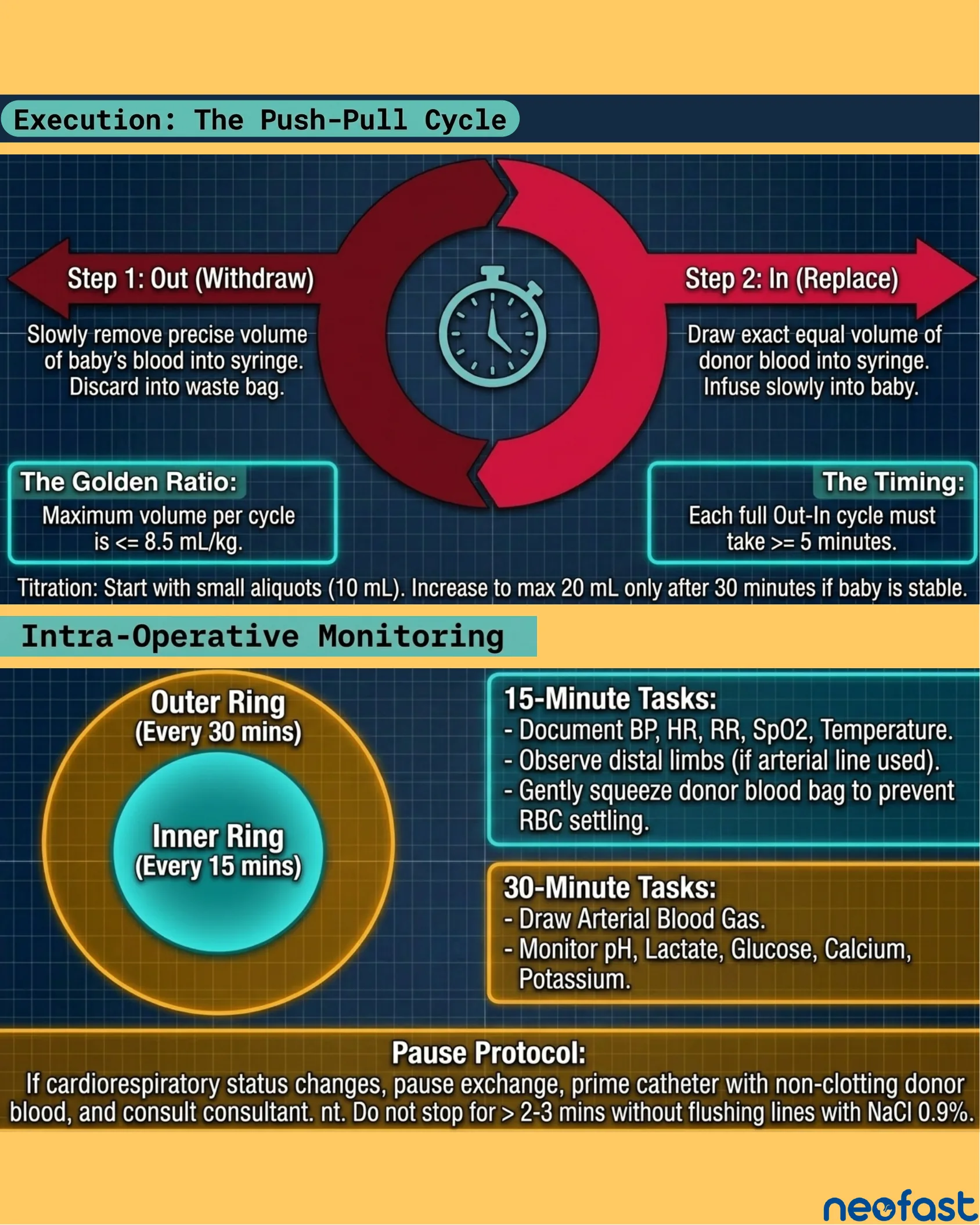
Execution: The Push-Pull Cycle
- Step 1: Out (Withdraw) – Slowly remove precise volume of baby’s blood into syringe. Discard into waste bag.
- Step 2: In (Replace) – Draw exact equal volume of donor blood into syringe. Infuse slowly into baby.
- The Golden Ratio: Maximum volume per cycle is <= 8.5 mL/kg.
- The Timing: Each full Out-In cycle must take >= 5 minutes.
Titration: Start with small aliquots (10 mL). Increase to max 20 mL only after 30 minutes if baby is stable.
Intra-Operative Monitoring
- Inner Ring (Every 15 mins) – 15-Minute Tasks: Document BP, HR, RR, SpO2, Temperature. Observe distal limbs (if arterial line used). Gently squeeze donor blood bag to prevent RBC settling.
- Outer Ring (Every 30 mins) – 30-Minute Tasks: Draw Arterial Blood Gas. Monitor pH, Lactate, Glucose, Calcium, Potassium.
Pause Protocol
If cardiorespiratory status changes, pause exchange, prime catheter with non-clotting donor blood, and consult consultant. Do not stop for > 2-3 mins without flushing lines with NaCl 0.9%.
The Complications Radar
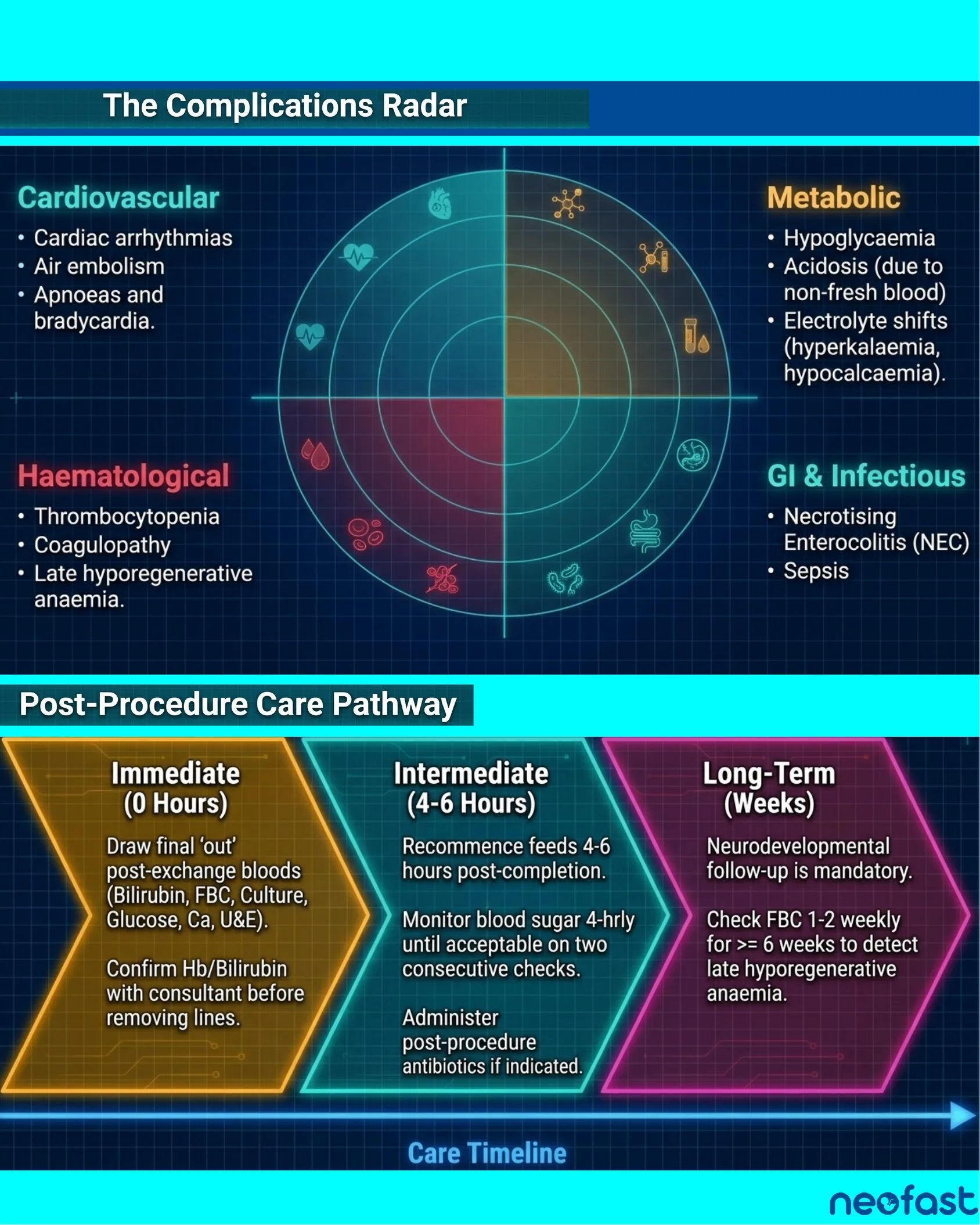
The Complications Radar
Cardiovascular
- Cardiac arrhythmias
- Air embolism
- Apnoeas and bradycardia.
Metabolic
- Hypoglycaemia
- Acidosis (due to non-fresh blood)
- Electrolyte shifts (hyperkalaemia, hypocalcaemia).
Haematological
- Thrombocytopenia
- Coagulopathy
- Late hyporegenerative anaemia.
GI & Infectious
- Necrotising Enterocolitis (NEC)
- Sepsis
Post-Procedure Care Pathway
- Immediate (0 Hours):
- Draw final ‘out’ post-exchange bloods (Bilirubin, FBC, Culture, Glucose, Ca, U&E).
- Confirm Hb/Bilirubin with consultant before removing lines.
- Intermediate (4-6 Hours):
- Recommence feeds 4-6 hours post-completion.
- Monitor blood sugar 4-hrly until acceptable on two consecutive checks.
- Administer post-procedure antibiotics if indicated.
- Long-Term (Weeks):
- Neurodevelopmental follow-up is mandatory.
- Check FBC 1-2 weekly for >= 6 weeks to detect late hyporegenerative anaemia.
Care Timeline
Synthesis: The Four Pillars of Exchange Transfusion
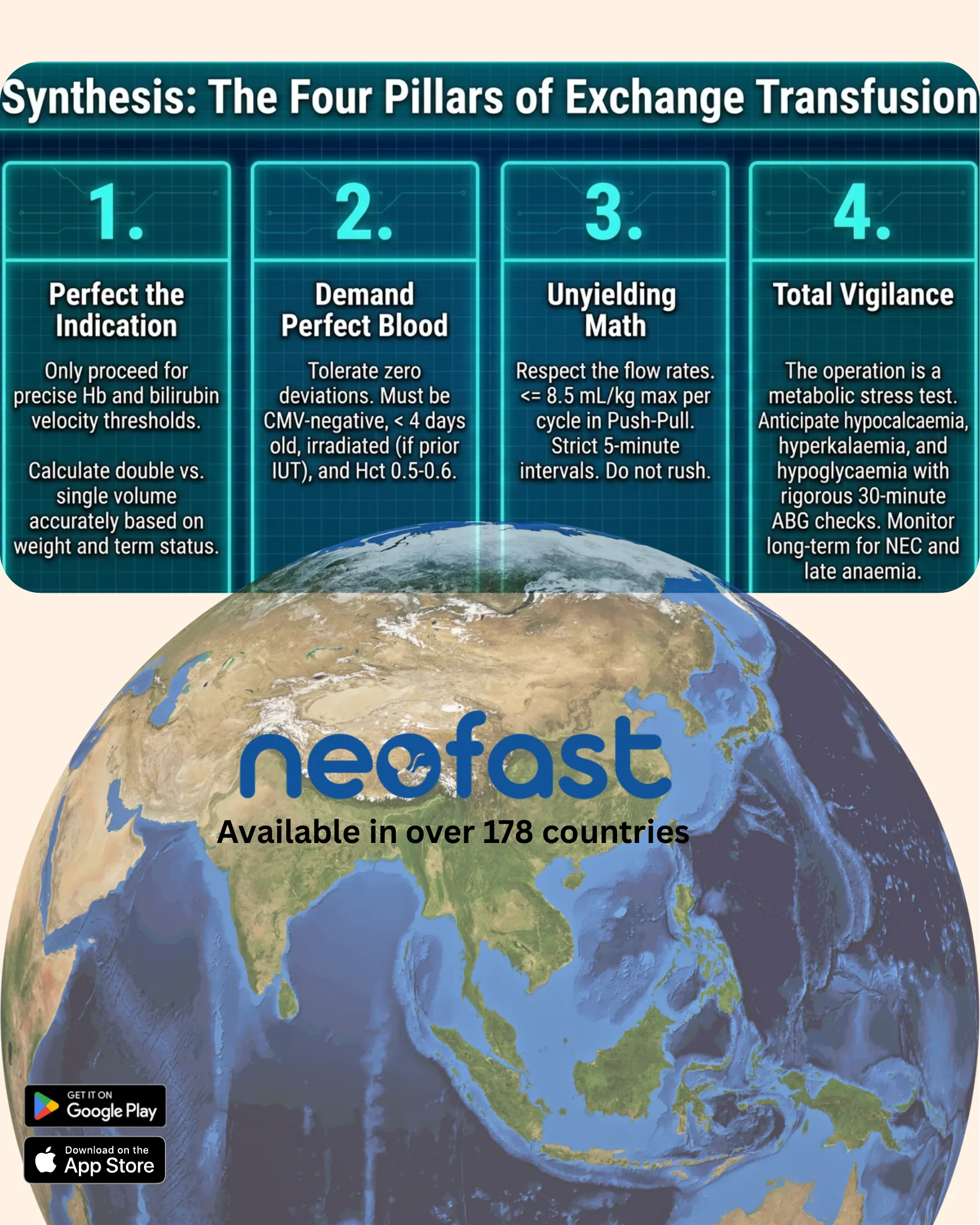
Synthesis: The Four Pillars of Exchange Transfusion
- Perfect the Indication
Only proceed for precise Hb and bilirubin velocity thresholds.
Calculate double vs. single volume accurately based on weight and term status.
- Demand Perfect Blood
Tolerate zero deviations. Must be CMV-negative, < 4 days old, irradiated (if prior IUT), and Hct 0.5-0.6.
- Unyielding Math
Respect the flow rates. <= 8.5 mL/kg max per cycle in Push-Pull. Strict 5-minute intervals. Do not rush.
- Total Vigilance
The operation is a metabolic stress test. Anticipate hypocalcaemia, hyperkalaemia, and hypoglycaemia with rigorous 30-minute ABG checks. Monitor long-term for NEC and late anaemia.
neofast — Available in over 178 countries
- Get it on Google Play
- Download on the App Store